

Early Medicaid Expansion and Cancer Mortality
- PMID: 34259321
- PMCID: PMC8634305
- DOI: 10.1093/jnci/djab135
Early Medicaid Expansion and Cancer Mortality
Abstract
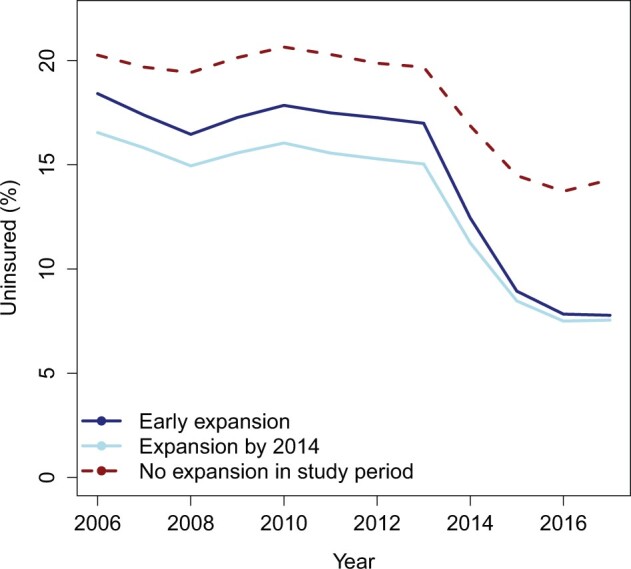
Background: Although Medicaid expansion is associated with decreased uninsured rates and earlier cancer diagnoses, no study has demonstrated an association between Medicaid expansion and cancer mortality. Our primary objective was to quantify the relationship between early Medicaid expansion and changes in cancer mortality rates.
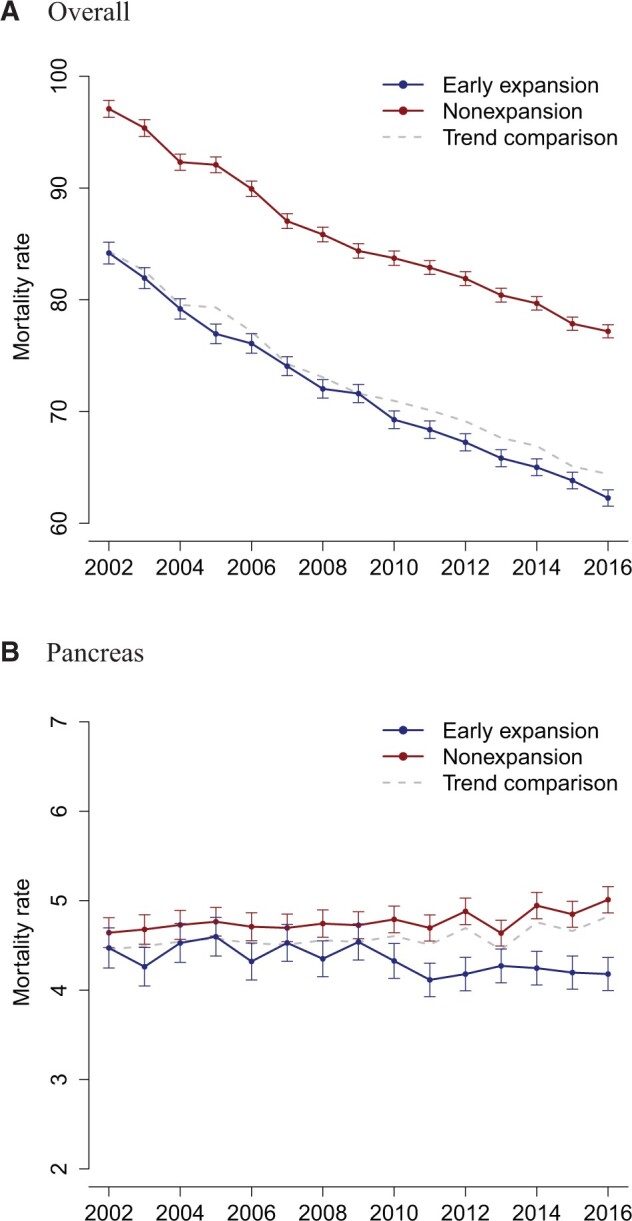
Methods: We obtained county-level data from the National Center for Health Statistics for adults aged 20-64 years who died from cancer from 2007 to 2009 (preexpansion) and 2012 to 2016 (postexpansion). We compared changes in cancer mortality rates in early Medicaid expansion states (CA, CT, DC, MN, NJ, and WA) vs nonexpansion states through a difference-in-differences analysis using hierarchical Bayesian regression. An exploratory analysis of cancer mortality changes associated with the larger-scale 2014 Medicaid expansions was also performed.
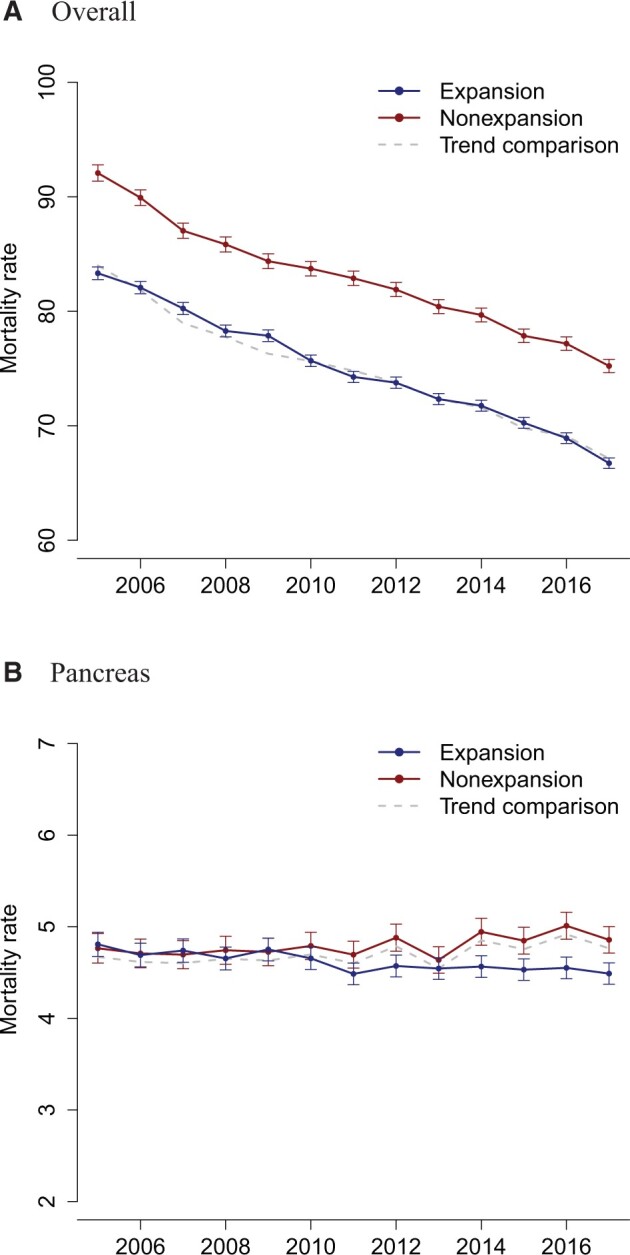
Results: In adjusted difference-in-differences analyses, we observed a statistically significant decrease of 3.07 (95% credible interval = 2.19 to 3.95) cancer deaths per 100 000 in early expansion vs nonexpansion states, which translates to an estimated decrease of 5276 cancer deaths in the early expansion states during the study period. Expansion-associated decreases in cancer mortality were observed for pancreatic cancer. Exploratory analyses of the 2014 Medicaid expansions showed a decrease in pancreatic cancer mortality (-0.18 deaths per 100 000, 95% confidence interval = -0.32 to -0.05) in states that expanded Medicaid by 2014 compared with nonexpansion states.
Conclusions: Early Medicaid expansion was associated with reduced cancer mortality rates, especially for pancreatic cancer, a cancer with short median survival where changes in prognosis would be most visible with limited follow-up.
© The Author(s) 2021. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
A First Look at Medicaid Expansion's Impact on Cancer Mortality Rates.J Natl Cancer Inst. 2021 Nov 29;113(12):1611-1612. doi: 10.1093/jnci/djab136. J Natl Cancer Inst. 2021. PMID: 34259325 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A.. Cancer statistics, 2020. CA A Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590. - PubMed
-
- Dimick JB, Ryan AM.. Methods for evaluating changes in health care policy: the difference-in-differences approach. JAMA. 2014;312(22):2401–2402. doi:10.1001/jama.2014. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
