

Optical coherence tomography angiography indicates subclinical retinal disease in neuromyelitis optica spectrum disorders
- PMID: 34259579
- PMCID: PMC8961243
- DOI: 10.1177/13524585211028831
Optical coherence tomography angiography indicates subclinical retinal disease in neuromyelitis optica spectrum disorders
Abstract
Background: Neuromyelitis optica spectrum disorders (NMOSD) are neuroinflammatory diseases of the central nervous system. Patients suffer from recurring relapses and it is unclear whether relapse-independent disease activity occurs and whether this is of clinical relevance.
Objective: To detect disease-specific alterations of the retinal vasculature that reflect disease activity during NMOSD.
Methods: Cross-sectional analysis of 16 patients with NMOSD, 21 patients with relapsing-remitting multiple sclerosis, and 21 healthy controls using retinal optical coherence tomography (OCT), optical coherence tomography angiography (OCT-A), measurement of glial fibrillary acidic protein (GFAP) serum levels, and assessment of visual acuity.
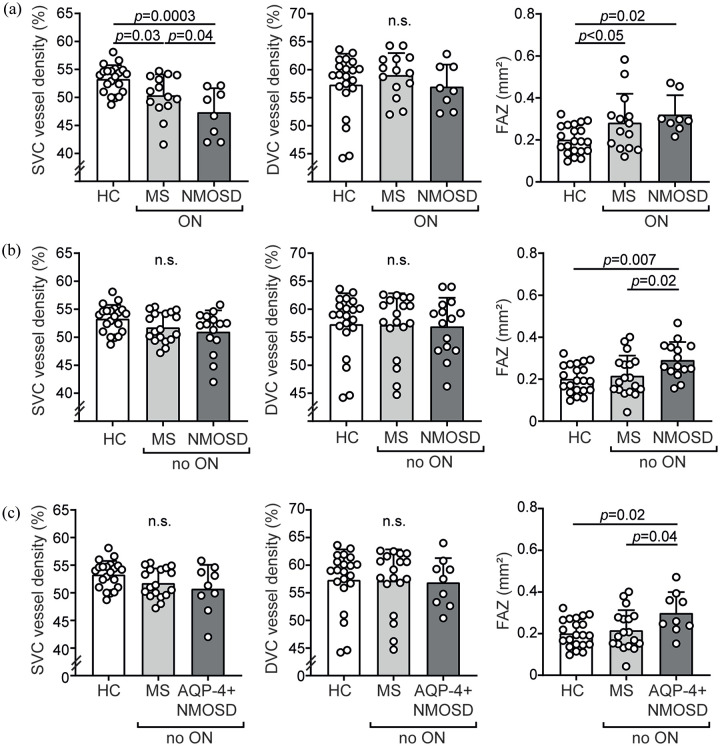
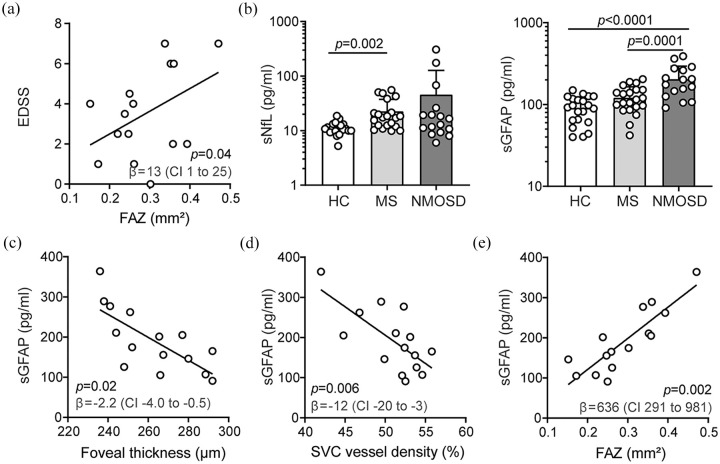
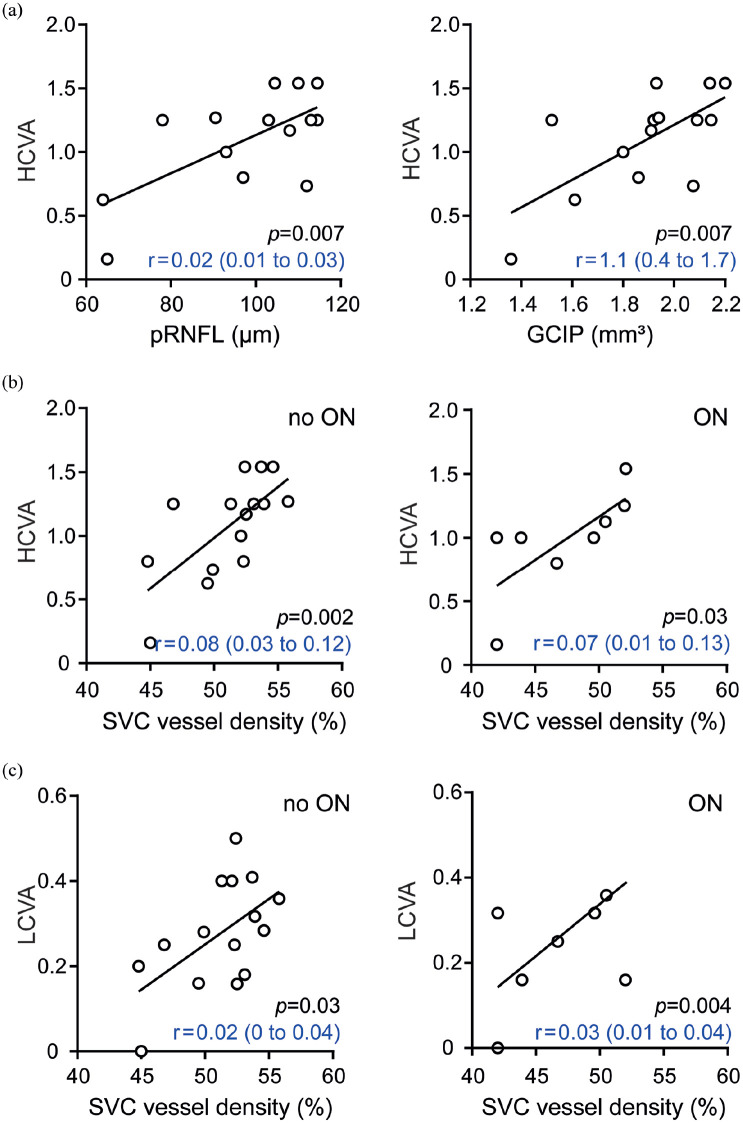
Results: Patients with NMOSD but not multiple sclerosis revealed lower foveal thickness (FT) (p = 0.02) measures and an increase of the foveal avascular zone (FAZ) (p = 0.02) compared to healthy controls independent to optic neuritis. Reduced FT (p = 0.01), enlarged FAZ areas (p = 0.0001), and vessel loss of the superficial vascular complex (p = 0.01) were linked to higher serum GFAP levels and superficial vessel loss was associated with worse visual performance in patients with NMOSD irrespective of optic neuritis.
Conclusion: Subclinical parafoveal retinal vessel loss might occur during NMOSD and might be linked to astrocyte damage and poor visual performance. OCT-A may be a tool to study subclinical disease activity during NMOSD.
Keywords: Neuromyelitis optica spectrum disorders; astrocytes; biomarker; disease activity; optical coherence tomography angiography.
Conflict of interest statement
Figures
References
-
- Jarius S, Paul F, Weinshenker BG, et al.. Neuromyelitis optica. Nat Rev Dis Primers 2020; 6: 85. - PubMed
-
- Roca-Fernandez A, Oertel FC, Yeo T, et al.. Foveal changes in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorder are independent of optic neuritis and not overtly progressive. Eur J Neurol 2021; 28(7): 2280–2293. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
