

Trends in ICU Mortality From Coronavirus Disease 2019: A Tale of Three Surges
- PMID: 34259667
- PMCID: PMC8796834
- DOI: 10.1097/CCM.0000000000005185
Trends in ICU Mortality From Coronavirus Disease 2019: A Tale of Three Surges
Abstract
Objectives: To determine the association between time period of hospitalization and hospital mortality among critically ill adults with coronavirus disease 2019.
Design: Observational cohort study from March 6, 2020, to January 31, 2021.
Setting: ICUs at four hospitals within an academic health center network in Atlanta, GA.
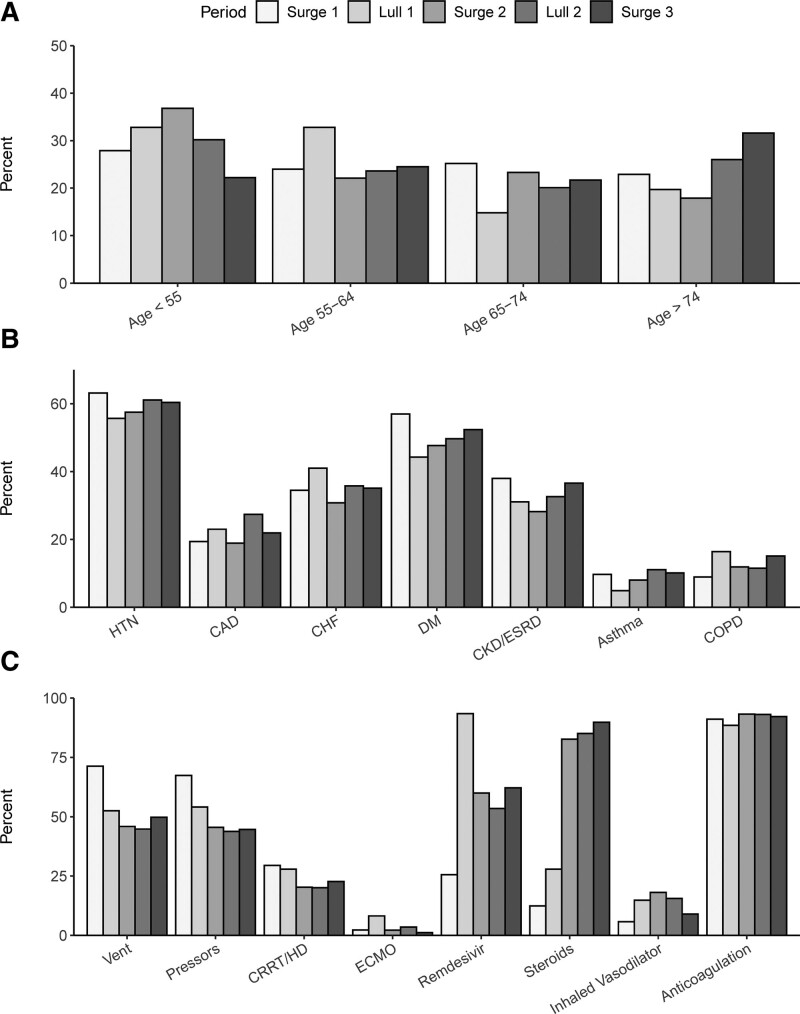
Patients: Adults greater than or equal to 18 years with coronavirus disease 2019 admitted to an ICU during the study period (i.e., Surge 1: March to April, Lull 1: May to June, Surge 2: July to August, Lull 2: September to November, Surge 3: December to January).
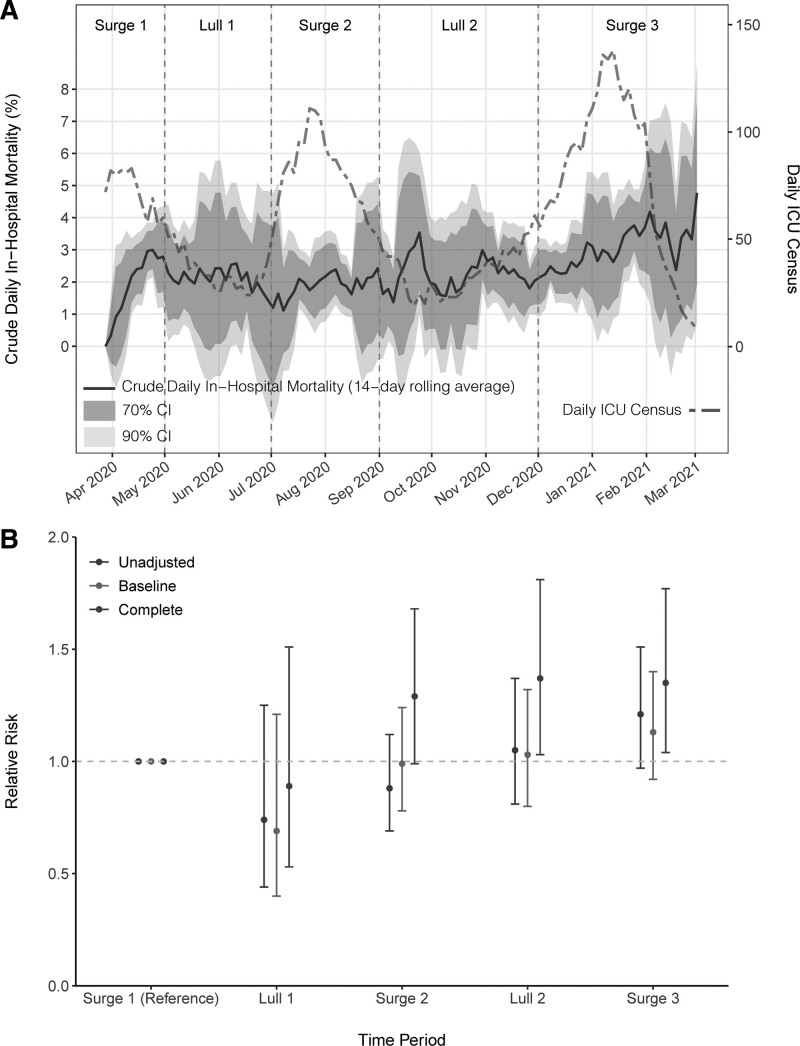
Measurements and main results: Among 1,686 patients with coronavirus disease 2019 admitted to an ICU during the study period, all-cause hospital mortality was 29.7%. Mortality differed significantly over time: 28.7% in Surge 1, 21.3% in Lull 1, 25.2% in Surge 2, 30.2% in Lull 2, 34.7% in Surge 3 (p = 0.007). Mortality was significantly associated with 1) preexisting risk factors (older age, race, ethnicity, lower body mass index, higher Elixhauser Comorbidity Index, admission from a nursing home); 2) clinical status at ICU admission (higher Sequential Organ Failure Assessment score, higher d-dimer, higher C-reactive protein); and 3) ICU interventions (receipt of mechanical ventilation, vasopressors, renal replacement therapy, inhaled vasodilators). After adjusting for baseline and clinical variables, there was a significantly increased risk of mortality associated with admission during Lull 2 (relative risk, 1.37 [95% CI = 1.03-1.81]) and Surge 3 (relative risk, 1.35 [95% CI = 1.04-1.77]) as compared to Surge 1.
Conclusions: Despite increased experience and evidence-based treatments, the risk of death for patients admitted to the ICU with coronavirus disease 2019 was highest during the fall and winter of 2020. Reasons for this increased mortality are not clear.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Auld received support for article research from the National Institutes of Health. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
