

Similar appearance of different multifocal carpal bone destructing disease entities in 3 patients: A case report
- PMID: 34260526
- PMCID: PMC8284703
- DOI: 10.1097/MD.0000000000026445
Similar appearance of different multifocal carpal bone destructing disease entities in 3 patients: A case report
Abstract
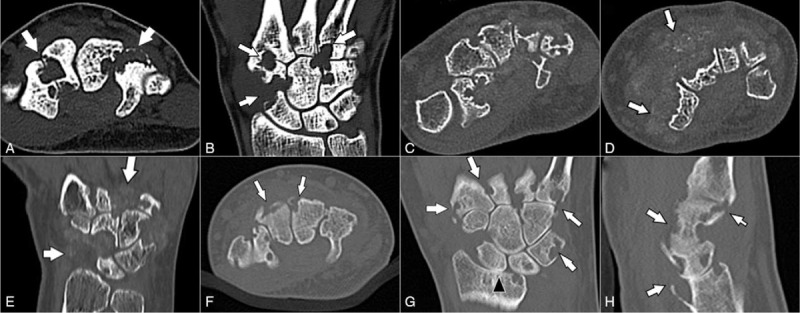
Rationale: Several diseases feature tumors, or tumor-mimicking lesions, that further invade the bone and surrounding joints of the wrist region. Here, we describe 3 rare cases of multiple destructed carpal bones and adjacent joints in different disease entities confirmed via pathologic diagnosis.
Patient concerns: All 3 cases were examined between January 2016 and December 2019. Three patients presented with similar clinical manifestations and radiographic features, with multiple osteolytic lesions in the carpal bones and metacarpal bone base.
Diagnoses: The 3 cases were diagnosed as diffuse type tenosynovial giant cell tumor, calcifying aponeurotic fibroma, and rheumatoid arthritis.
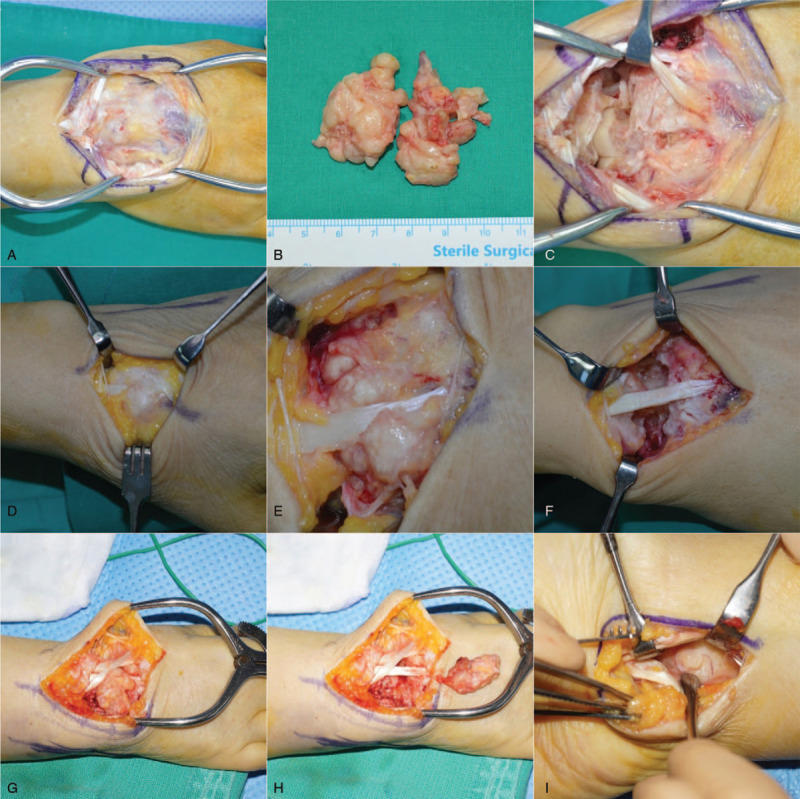
Interventions: Separate, experienced radiologist and pathologist took part in the interpretation and compartmentalization of radiographs and pathological findings, respectively. Even magnetic resonance imaging could not achieve a diagnosis; surgical excision was therefore required, with subsequent pathological assessment for treatment and final diagnosis.
Outcomes: functional outcomes also differed among patients, poorest in rheumatoid arthritis patient.
Lessons: We report 3 rare disease entities, presenting with multifocal osteolytic lesions in the wrist. They all presented with similar clinical manifestations, and the final diagnoses were made via pathological evaluation. Compared with tenosynovial giant cell tumor and calcifying aponeurotic fibroma, rheumatoid arthritis had the poorest outcome.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures



References
-
- Garcia-Elias M, Lluch AL. Cohen MS, Green DP, Hotchkiss RN, Kozin SH, Pederson WC, Wolfe SW. Wrist instabilities, misalignments, and dislocations. Green's Operative Hand Surgery.. Philadelphia, PA: Elsevier; 2017. 418–78.
-
- Zhao X, Qi C, Chen J, et al. . Synovial hemangioma of the wrist with cystic invasion of trapezoid and capitate bones. J Hand Surg Am 2020;45:161.e1–e6. - PubMed
-
- Lee SM, Ha DH, Kang H, et al. . Intraarticular calcifying aponeurotic fibroma of the wrist: mimicking gout or calcium pyrophosphate dihydrate deposition disease. Skeletal Radiol 2018;47:729–34. - PubMed
-
- Athanasian EA. Cohen MS, Green DP, Hotchkiss RN, Kozin SH, Pederson WC, Wolfe SW. Bone and soft tissue tumors. Green's Operative Hand Surgery. Philadelphia, PA: Elsevier; 2017. 1987–2035.
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
