

Approach to the Patient With Adrenal Incidentaloma
- PMID: 34260734
- PMCID: PMC8530736
- DOI: 10.1210/clinem/dgab512
Approach to the Patient With Adrenal Incidentaloma
Abstract
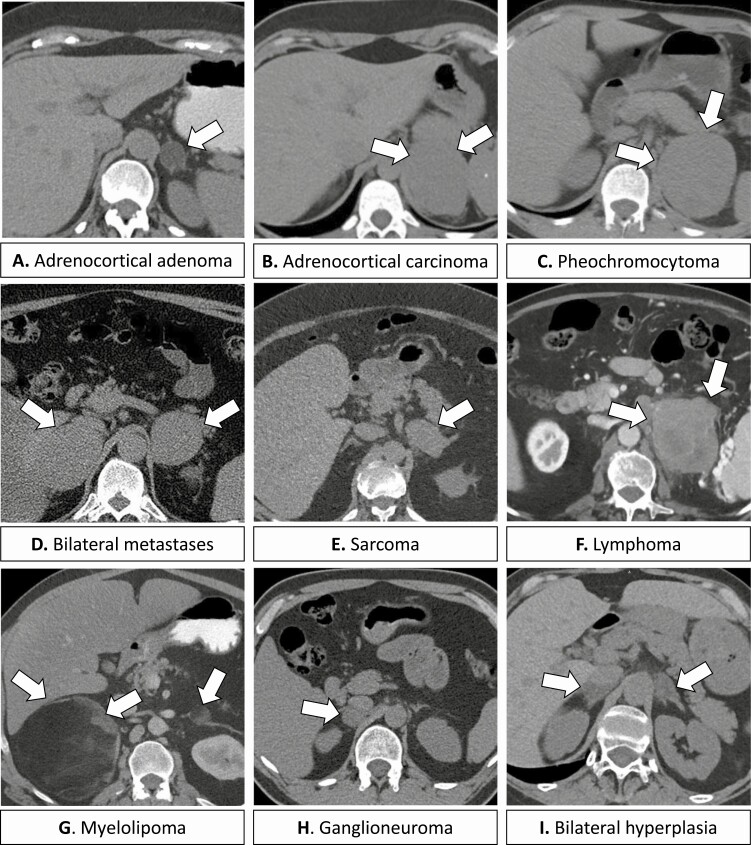
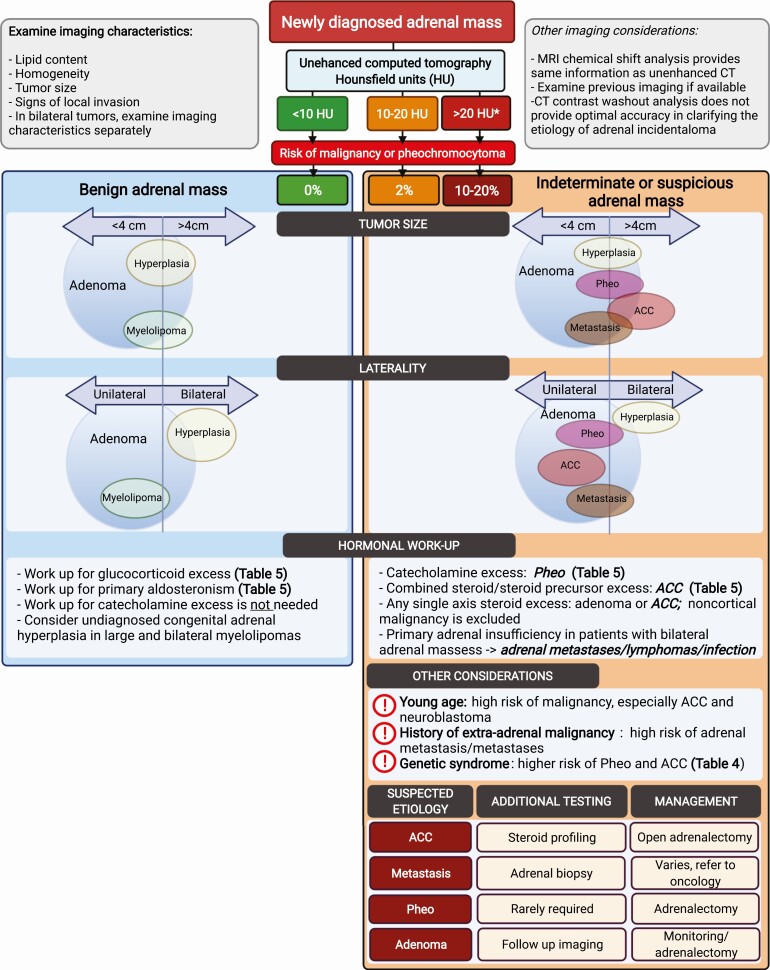
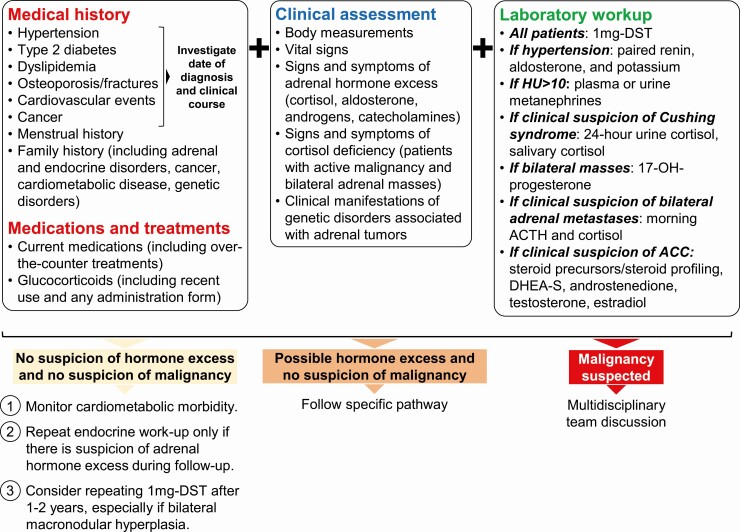
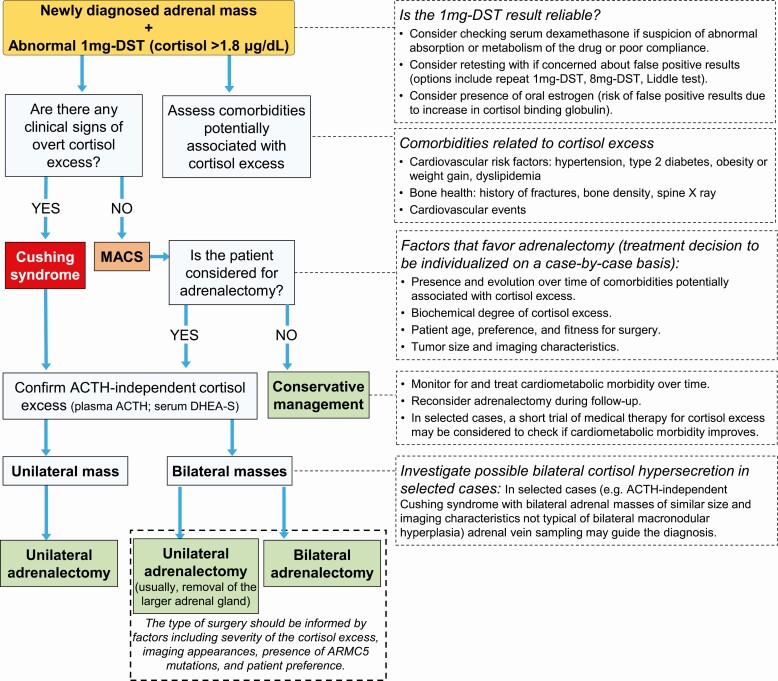
Adrenal tumors are commonly discovered incidentally on cross-sectional abdominal imaging performed for reasons other than adrenal mass. Incidence of adrenal tumors increased 10-fold in the past 2 decades, with most diagnosed in older adults. In any patient with a newly discovered adrenal mass, determining whether the adrenal mass is malignant and whether it is hormonally active is equally important to guide the best management. Malignancy is diagnosed in 5% to 8% of patients with adrenal tumors, with a higher risk in young patients, if history of extra-adrenal malignancy, in those with large adrenal tumors with indeterminate imaging characteristics, and in bilateral adrenal tumors. Although overt hormone excess is uncommon in adrenal incidentalomas, mild autonomous cortisol secretion can be diagnosed in up to 30% to 50% of patients. Because autonomous cortisol secretion is associated with increased cardiovascular morbidity and metabolic abnormalities, all patients with adrenal incidentalomas require work up with dexamethasone suppression test. Management of adrenal tumors varies based on etiology, associated comorbidities, and patient's preference. This article reviews the current evidence on the diagnosis and evaluation of patients with adrenal mass and focuses on management of the most common etiologies of adrenal incidentalomas.
Keywords: Hounsfield units; adrenal mass; dexamethasone suppression test; diagnosis; hormonal work up; imaging; malignancy.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Reimondo G, Castellano E, Grosso M, et al. Adrenal incidentalomas are tied to increased risk of diabetes: findings from a prospective study. J Clin Endocrinol Metab. 2020;105(4):e973-e981. - PubMed
-
- Ichijo T, Ueshiba H, Nawata H, Yanase T. A nationwide survey of adrenal incidentalomas in Japan: the first report of clinical and epidemiological features. Endocr J. 2020;67(2):141-152. - PubMed
-
- Mantero F, Terzolo M, Arnaldi G, et al. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J Clin Endocrinol Metab. 2000;85(2):637-644. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
