

The CoVID-TE risk assessment model for venous thromboembolism in hospitalized patients with cancer and COVID-19
- PMID: 34260813
- PMCID: PMC8420489
- DOI: 10.1111/jth.15463
The CoVID-TE risk assessment model for venous thromboembolism in hospitalized patients with cancer and COVID-19
Erratum in
-
Corrigendum.J Thromb Haemost. 2022 Mar;20(3):785-786. doi: 10.1111/jth.15627. J Thromb Haemost. 2022. PMID: 35220657 Free PMC article. No abstract available.
Abstract
Background: Hospitalized patients with COVID-19 have increased risks of venous (VTE) and arterial thromboembolism (ATE). Active cancer diagnosis and treatment are well-known risk factors; however, a risk assessment model (RAM) for VTE in patients with both cancer and COVID-19 is lacking.
Objectives: To assess the incidence of and risk factors for thrombosis in hospitalized patients with cancer and COVID-19.
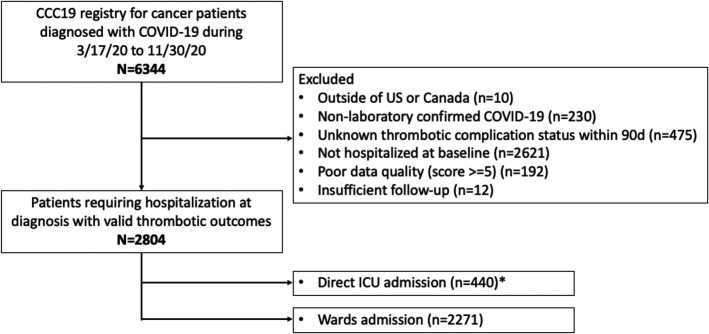
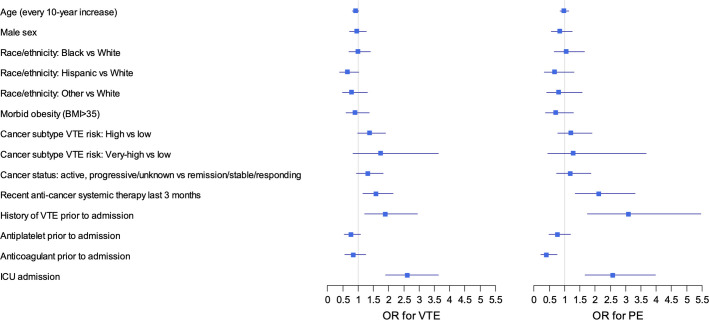
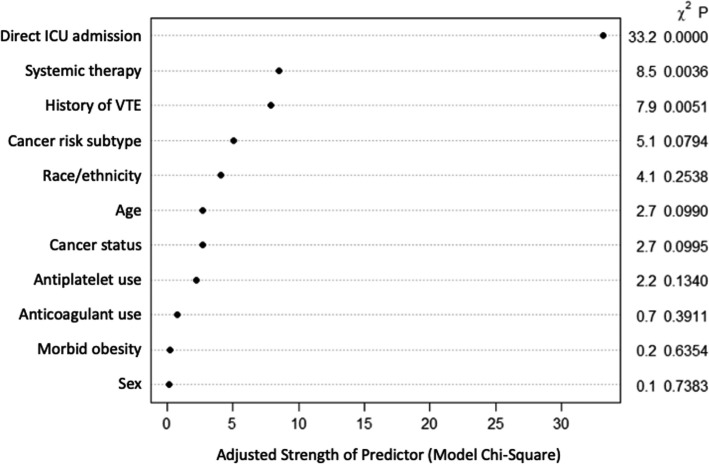
Methods: Among patients with cancer in the COVID-19 and Cancer Consortium registry (CCC19) cohort study, we assessed the incidence of VTE and ATE within 90 days of COVID-19-associated hospitalization. A multivariable logistic regression model specifically for VTE was built using a priori determined clinical risk factors. A simplified RAM was derived and internally validated using bootstrap.
Results: From March 17, 2020 to November 30, 2020, 2804 hospitalized patients were analyzed. The incidence of VTE and ATE was 7.6% and 3.9%, respectively. The incidence of VTE, but not ATE, was higher in patients receiving recent anti-cancer therapy. A simplified RAM for VTE was derived and named CoVID-TE (Cancer subtype high to very-high risk by original Khorana score +1, VTE history +2, ICU admission +2, D-dimer elevation +1, recent systemic anti-cancer Therapy +1, and non-Hispanic Ethnicity +1). The RAM stratified patients into two cohorts (low-risk, 0-2 points, n = 1423 vs. high-risk, 3+ points, n = 1034) where VTE occurred in 4.1% low-risk and 11.3% high-risk patients (c statistic 0.67, 95% confidence interval 0.63-0.71). The RAM performed similarly well in subgroups of patients not on anticoagulant prior to admission and moderately ill patients not requiring direct ICU admission.
Conclusions: Hospitalized patients with cancer and COVID-19 have elevated thrombotic risks. The CoVID-TE RAM for VTE prediction may help real-time data-driven decisions in this vulnerable population.
Keywords: COVID-19; SARS-CoV-2; clinical decision rules; thrombosis; venous thromboembolism.
© 2021 The Authors. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
