

Distinctive features of SARS-CoV-2-specific T cells predict recovery from severe COVID-19
- PMID: 34260965
- PMCID: PMC8238659
- DOI: 10.1016/j.celrep.2021.109414
Distinctive features of SARS-CoV-2-specific T cells predict recovery from severe COVID-19
Abstract
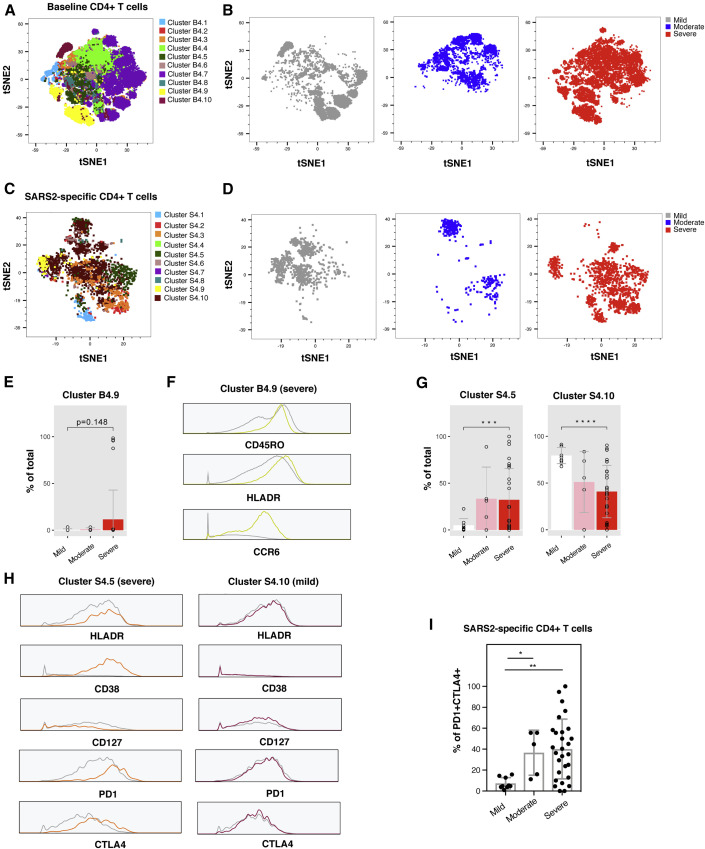
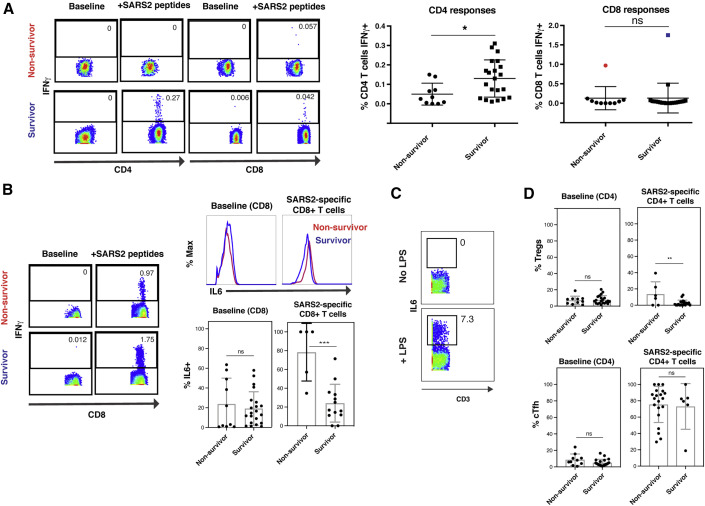
Although T cells are likely players in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) immunity, little is known about the phenotypic features of SARS-CoV-2-specific T cells associated with recovery from severe coronavirus disease 2019 (COVID-19). We analyze T cells from 34 individuals with COVID-19 with severity ranging from mild (outpatient) to critical, culminating in death. Relative to individuals who succumbed, individuals who recovered from severe COVID-19 harbor elevated and increasing numbers of SARS-CoV-2-specific T cells capable of homeostatic proliferation. In contrast, fatal COVID-19 cases display elevated numbers of SARS-CoV-2-specific regulatory T cells and a time-dependent escalation in activated bystander CXCR4+ T cells, as assessed by longitudinal sampling. Together with the demonstration of increased proportions of inflammatory CXCR4+ T cells in the lungs of individuals with severe COVID-19, these results support a model where lung-homing T cells activated through bystander effects contribute to immunopathology, whereas a robust, non-suppressive SARS-CoV-2-specific T cell response limits pathogenesis and promotes recovery from severe COVID-19.
Keywords: CD127; COVID-19; CXCR4; SARS-CoV-2; T cells; lung.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing financial interests.
Figures






Update of
-
Distinctive features of SARS-CoV-2-specific T cells predict recovery from severe COVID-19.medRxiv [Preprint]. 2021 Feb 5:2021.01.22.21250054. doi: 10.1101/2021.01.22.21250054. medRxiv. 2021. Update in: Cell Rep. 2021 Jul 20;36(3):109414. doi: 10.1016/j.celrep.2021.109414. PMID: 33532792 Free PMC article. Updated. Preprint.
References
-
- Anft M., Paniskaki K., Blazquez-Navarro A., Doevelaar A., Seibert F.S., Hoelzer B., Skrzypczyk S., Kohut E., Kurek J., Zapka J. COVID-19 progression is potentially driven by T cell immunopathogenesis. medRxiv. 2020 doi: 10.1101/2020.04.28.20083089. - DOI
-
- Bastard P., Rosen L.B., Zhang Q., Michailidis E., Hoffmann H.H., Zhang Y., Dorgham K., Philippot Q., Rosain J., Béziat V., HGID Lab. NIAID-USUHS Immune Response to COVID Group. COVID Clinicians. COVID-STORM Clinicians. Imagine COVID Group. French COVID Cohort Study Group. Milieu Intérieur Consortium. CoV-Contact Cohort. Amsterdam UMC Covid-19 Biobank. COVID Human Genetic Effort Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science. 2020;370:eabd4585. - PMC - PubMed
-
- Braun J., Loyal L., Frentsch M., Wendisch D., Georg P., Kurth F., Hippenstiel S., Dingeldey M., Kruse B., Fauchere F. SARS-CoV-2-reactive T cells in healthy donors and patients with COVID-19. Nature. 2020;587:270–274. - PubMed
-
- Cashen A.F., Nervi B., DiPersio J. AMD3100: CXCR4 antagonist and rapid stem cell-mobilizing agent. Future Oncol. 2007;3:19–27. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
