

Salvage of severe knee osteoarthritis: efficacy of tibial condylar valgus osteotomy versus open wedge high tibial osteotomy
- PMID: 34261504
- PMCID: PMC8278751
- DOI: 10.1186/s13018-021-02597-x
Salvage of severe knee osteoarthritis: efficacy of tibial condylar valgus osteotomy versus open wedge high tibial osteotomy
Abstract
Introduction: To compare the clinical outcomes and the radiographic features between tibial condylar valgus osteotomy (TCVO) and open wedge high tibial osteotomy (OWHTO). New insight into the indication criteria for TCVO was also clarified for achieving satisfactory results.
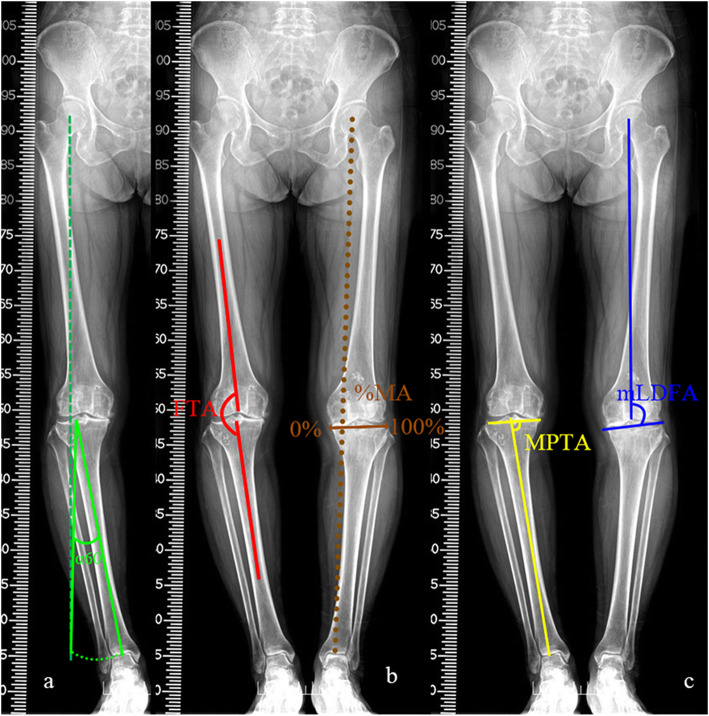
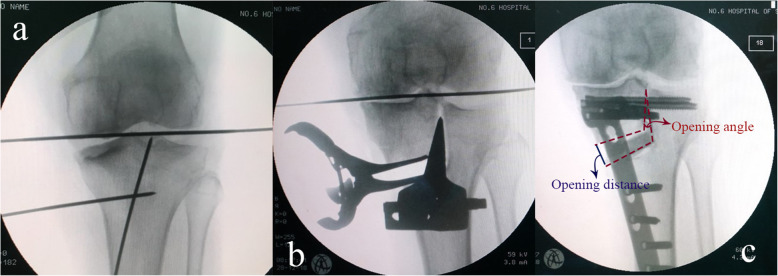
Materials and methods: Sixty-three knees with medial-compartment osteoarthritis were retrospectively studied. Thirty-four knees with subluxated lateral joint and depression of the medial tibial plateau underwent TCVO and the rest underwent OWHTO. Among the 63 knees included, 27 knees with a pre-operative femorotibial angle (FTA) ≥ 185° were defined as severe varus (subgroup S, 15 in STCVO group and 12 in SHTO group). Lower limb alignment, intra-, and extra-articular congruency were evaluated according to the radiograph obtained before and 24 months after surgery. The visual analog scale (VAS) score and Hospital for Special Surgery (HSS) score were obtained to assess the clinical results. Opening angle and distance of the opening gap in each group were measured by intra-operative fluoroscopy.
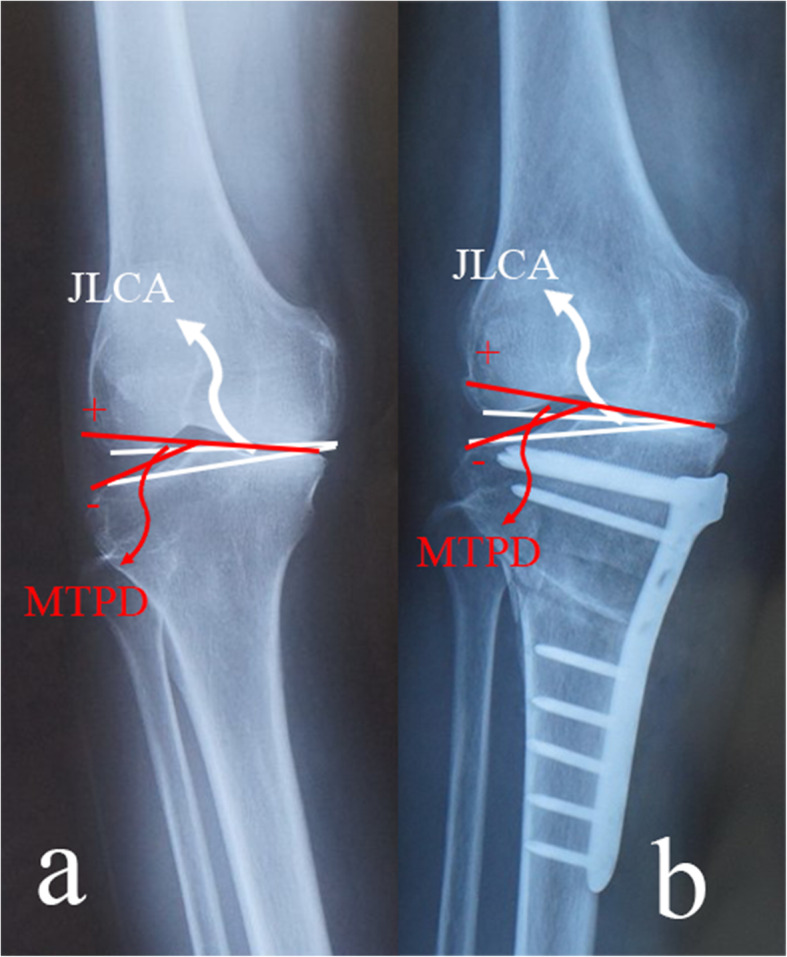
Results: During the 2-year follow-up period, the mean HSS score increased from 70.3 to 81.4 in HTO group and 65.9 to 87.3 in TCVO group (p < 0.05). The mean VAS score decreased from 5.9 to 2.6 and 6.0 to 2.1, respectively (p < 0.01). Pre-operative FTA was restored to 172.9° in HTO group and 171.3° in TCVO group, and percentage of mechanical axis (%MA) was improved to 59.7% and 61.2%, respectively. Joint line convergence angle (JLCA) was slightly restored and medial tibial plateau depression (MTPD) was relatively the same before and after OWHTO, while these parameters improved greatly (from 6.4° to 1.2° and - 8.0° to 5.9°, p < 0.01) in TCVO group. More undercorrected knees were observed in SHTO group than STCVO group (58.3% and 13.3%, p < 0.05). Opening angle and distance of the opening gap were larger in TCVO group (19.1° and 14.0 mm) than those in OWHTO group (9.3° and 10.1 mm, p < 0.05).
Conclusion: Compared to OWHTO, TCVO had priority in treating advanced knee OA with intra-articular deformity. However, TCVO had a limited capacity to correct the varus angle. Besides, TCVO might be suitable for medial-compartment OA with a pre-operative FTA ≥ 185°.
Keywords: Open wedge high tibial osteotomy (OWHTO); Osteoarthritis (OA); Tibial condylar valgus osteotomy (TCVO).
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Comparison of short-term clinical outcomes between open-wedge high tibial osteotomy and tibial condylar valgus osteotomy.BMC Musculoskelet Disord. 2024 Jan 27;25(1):98. doi: 10.1186/s12891-024-07205-7. BMC Musculoskelet Disord. 2024. PMID: 38281004 Free PMC article.
-
Tibial condylar valgus osteotomy (TCVO) for osteoarthritis of the knee: 5-year clinical and radiological results.Arch Orthop Trauma Surg. 2017 Mar;137(3):303-310. doi: 10.1007/s00402-016-2609-3. Epub 2017 Jan 28. Arch Orthop Trauma Surg. 2017. PMID: 28132085 Free PMC article.
-
Association of Preoperative Tibial Varus Deformity With Joint Line Orientation and Clinical Outcome After Open-Wedge High Tibial Osteotomy for Medial Compartment Osteoarthritis: A Propensity Score-Matched Analysis.Am J Sports Med. 2021 Nov;49(13):3551-3560. doi: 10.1177/03635465211044146. Epub 2021 Oct 8. Am J Sports Med. 2021. PMID: 34623942
-
Intra- and Extra-Articular Deformity of Lower Limb: Tibial Condylar Valgus Osteotomy (TCVO) and Distal Tibial Oblique Osteotomy (DTOO) for Reconstruction of Joint Congruency.Adv Orthop. 2019 Feb 18;2019:8605674. doi: 10.1155/2019/8605674. eCollection 2019. Adv Orthop. 2019. PMID: 30906598 Free PMC article. Review.
-
Is opening-wedge high tibial osteotomy superior to closing-wedge high tibial osteotomy in treatment of unicompartmental osteoarthritis? A meta-analysis of randomized controlled trials.Int J Surg. 2018 Dec;60:153-163. doi: 10.1016/j.ijsu.2018.10.045. Epub 2018 Nov 13. Int J Surg. 2018. PMID: 30445197 Review.
Cited by
-
Geometrical analysis of the opening gap after tibial condylar valgus osteotomy for proper hinge point selection.Ann Transl Med. 2022 Dec;10(23):1267. doi: 10.21037/atm-22-2022. Ann Transl Med. 2022. PMID: 36618801 Free PMC article.
-
Digitized Precision Corrective Osteotomy for Treating Knee Joint Deformities: Current Evidence and Future Perspectives.Orthop Surg. 2025 Aug;17(8):2221-2233. doi: 10.1111/os.70085. Epub 2025 May 29. Orthop Surg. 2025. PMID: 40441744 Free PMC article. Review.
-
Coronal Plane Alignment of the Knee (CPAK) Type Shifts Toward Constitutional Varus with Increasing Kellgren and Lawrence Grade: A Radiographic Analysis of 17,365 Knees.J Bone Joint Surg Am. 2024 Dec 24;107(3):297-303. doi: 10.2106/JBJS.24.00316. Online ahead of print. J Bone Joint Surg Am. 2024. PMID: 39719004 Free PMC article.
-
High tibial osteotomy improves balance control in patients with knee osteoarthritis and a varus deformity.J Orthop Surg Res. 2023 Jul 28;18(1):538. doi: 10.1186/s13018-023-04041-8. J Orthop Surg Res. 2023. PMID: 37507811 Free PMC article.
-
Effects of K-wire diameter and insertion angle on femoral bone medial closing-wedge osteotomies: a finite element study.Sci Rep. 2025 Jun 20;15(1):20116. doi: 10.1038/s41598-025-04260-5. Sci Rep. 2025. PMID: 40541981 Free PMC article.
References
-
- Hochberg MC, Altman RD, Brandt KD, Clark BM, Dieppe PA, Griffin MR, Moskowitz RW, Schnitzer TJ. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum. 1995;38(11):1541–1546. doi: 10.1002/art.1780381104. - DOI - PubMed
-
- Smith WB, 2nd, Steinberg J, Scholtes S, McNamara IR. Medial compartment knee osteoarthritis: age-stratified cost-effectiveness of total knee arthroplasty, unicompartmental knee arthroplasty, and high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2017;25(3):924–933. doi: 10.1007/s00167-015-3821-3. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
