

Isolated Adrenocorticotropic Hormone Deficiency Associated with Severe Hyperkalemia During Pembrolizumab Therapy in a Patient with Ureteral Cancer and an Ileal Conduit: A Case Report and Literature Review
- PMID: 34262010
- PMCID: PMC8297058
- DOI: 10.12659/AJCR.931639
Isolated Adrenocorticotropic Hormone Deficiency Associated with Severe Hyperkalemia During Pembrolizumab Therapy in a Patient with Ureteral Cancer and an Ileal Conduit: A Case Report and Literature Review
Abstract
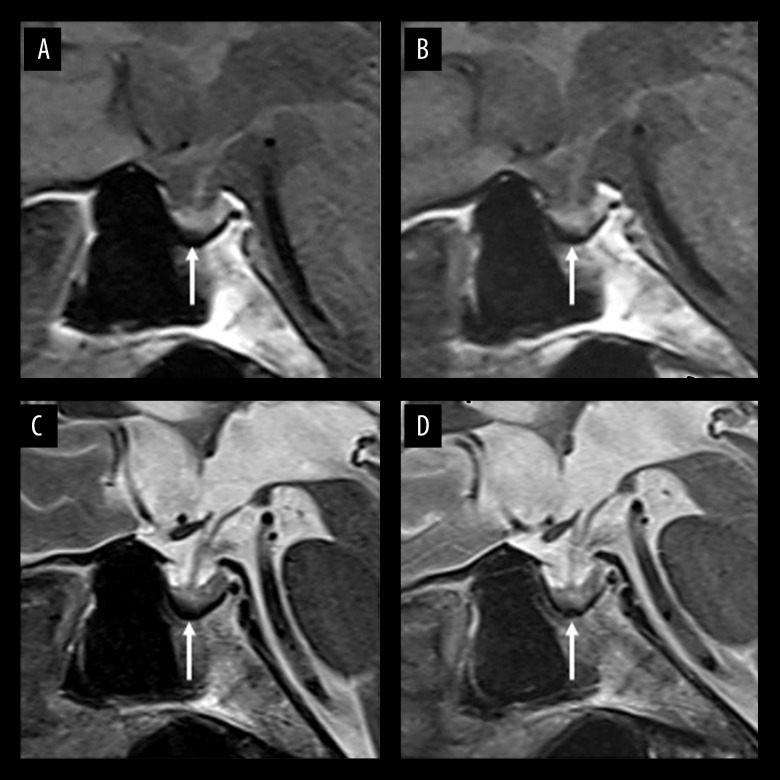
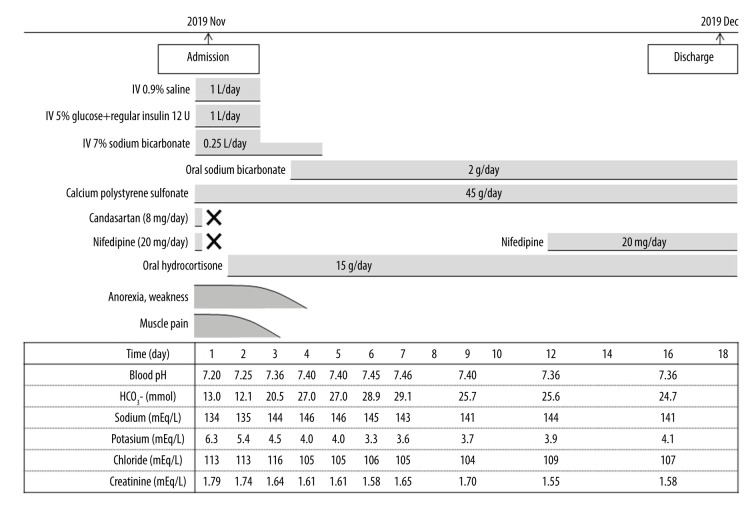
BACKGROUND Immune checkpoint inhibitors (ICIs) are anticancer medications that enhance the antitumor immune response. The clinical benefit afforded by ICIs, however, can be accompanied by immune-related adverse events (IRAEs). One of the common endocrine IRAEs is hypophysitis, which often causes hypopituitarism with secondary adrenal insufficiency (AI). Secondary AI, including isolated adrenocorticotropic hormone (ACTH) deficiency (IAD), is often associated with hyponatremia. Here, we report an unusual case of ICI-related IAD associated with severe hyperkalemia. CASE REPORT A 78-year-old woman who had an ileal conduit, chronic kidney disease, type 2 diabetes mellitus, and hypertension and was taking an angiotensin II receptor blocker began treatment for advanced ureteral cancer with the anti-programmed cell death protein 1 inhibitor pembrolizumab. The therapy effectively controlled the cancer, but 4 1/2 months after starting it, the patient developed anorexia, general weakness, and muscle pain and was diagnosed with IAD associated with severe hyperkalemia and hyperchloremic metabolic acidosis. She recovered after prompt administration of corticosteroids and treatment with sodium bicarbonate, glucose/insulin, and cation exchange resins. CONCLUSIONS Hyperkalemia is a common symptom of primary AI but is less common in patients with central AI because a lack of ACTH does not cause aldosterone deficiency and mineralocorticoid action is preserved. The present case demonstrates the need for physicians to be aware of severe hyperkalemia as a life-threatening complication of secondary AI induced by ICIs, particularly in patients with predisposing factors, such as kidney dysfunction, diabetes mellitus, an ileal conduit, and renin-angiotensin-aldosterone system inhibitor use.
Conflict of interest statement
None.
Figures
Similar articles
-
Isolated adrenocorticotropic hormone deficiency associated with sintilimab therapy in a patient with advanced lung adenocarcinoma: a case report and literature review.BMC Endocr Disord. 2022 Sep 24;22(1):239. doi: 10.1186/s12902-022-01151-y. BMC Endocr Disord. 2022. PMID: 36153581 Free PMC article. Review.
-
[Pituitary immune-related adverse events induced by programmed cell death protein 1 inhibitors in advanced lung cancer patients: A report of 3 cases].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Apr 18;54(2):369-375. doi: 10.19723/j.issn.1671-167X.2022.02.027. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35435206 Free PMC article. Chinese.
-
Isolated adrenocorticotropic hormone deficiency and thyroiditis associated with nivolumab therapy in a patient with advanced lung adenocarcinoma: a case report and review of the literature.J Med Case Rep. 2019 Mar 26;13(1):88. doi: 10.1186/s13256-019-2002-2. J Med Case Rep. 2019. PMID: 30909965 Free PMC article. Review.
-
Pembrolizumab- and ipilimumab-induced diabetic ketoacidosis and isolated adrenocorticotropic hormone deficiency: a case report.J Med Case Rep. 2020 Sep 29;14(1):171. doi: 10.1186/s13256-020-02502-w. J Med Case Rep. 2020. PMID: 32988414 Free PMC article.
-
Immune checkpoint inhibitors and adrenal insufficiency: a large-sample case series study.Ann Transl Med. 2022 Mar;10(5):251. doi: 10.21037/atm-21-7006. Ann Transl Med. 2022. PMID: 35402601 Free PMC article.
Cited by
-
Slowly Progressive Secondary Adrenal Insufficiency Due to Pembrolizumab Administration in a Patient With a History of Pituitary Neuroendocrine Tumor.Cureus. 2025 Mar 31;17(3):e81495. doi: 10.7759/cureus.81495. eCollection 2025 Mar. Cureus. 2025. PMID: 40308384 Free PMC article.
-
Immune checkpoint inhibitor-induced isolated adrenocorticotropic hormone deficiency: a systematic review.Front Endocrinol (Lausanne). 2024 Jan 22;15:1326684. doi: 10.3389/fendo.2024.1326684. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38318292 Free PMC article.
-
Machine Learning Models Using Routinely Collected Clinical Data Offer Robust and Interpretable Predictions of 90-Day Unplanned Acute Care Use for Cancer Immunotherapy Patients.JCO Clin Cancer Inform. 2023 Mar;7:e2200123. doi: 10.1200/CCI.22.00123. JCO Clin Cancer Inform. 2023. PMID: 37001039 Free PMC article.
-
Exploring a New Entity of Single-Agent Pembrolizumab-Associated Hypophysitis.Cureus. 2022 Aug 7;14(8):e27763. doi: 10.7759/cureus.27763. eCollection 2022 Aug. Cureus. 2022. PMID: 36127991 Free PMC article.
-
PD-1/PD-L1 inhibitor-induced hyponatremia: a real-world pharmacovigilance analysis using FAERS database.Front Immunol. 2025 Jun 16;16:1561942. doi: 10.3389/fimmu.2025.1561942. eCollection 2025. Front Immunol. 2025. PMID: 40589736 Free PMC article.
References
-
- Sznol M, Postow MA, Davies MJ, et al. Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treat Rev. 2017;58:70–76. - PubMed
-
- Faje A, Reynolds K, Zubiri L, et al. Hypophysitis secondary to nivolumab and pembrolizumab is a clinical entity distinct from ipilimumab-associated hypophysitis. Eur J Endocrinol. 2019;181:211–19. - PubMed
-
- Andrioli M, Pecori Giraldi F, Cavagnini F. Isolated corticotrophin deficiency. Pituitary. 2006;9:289–95. - PubMed
-
- Percik R, Shlomai G, Tirosh A, et al. Isolated autoimmune adrenocortico-tropic hormone deficiency: From a rare disease to the dominant cause of adrenal insufficiency related to check point inhibitors. Autoimmun Rev. 2020;19:102454. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
