

Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination
- PMID: 34262158
- PMCID: PMC8440184
- DOI: 10.1038/s41591-021-01449-9
Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination
Abstract
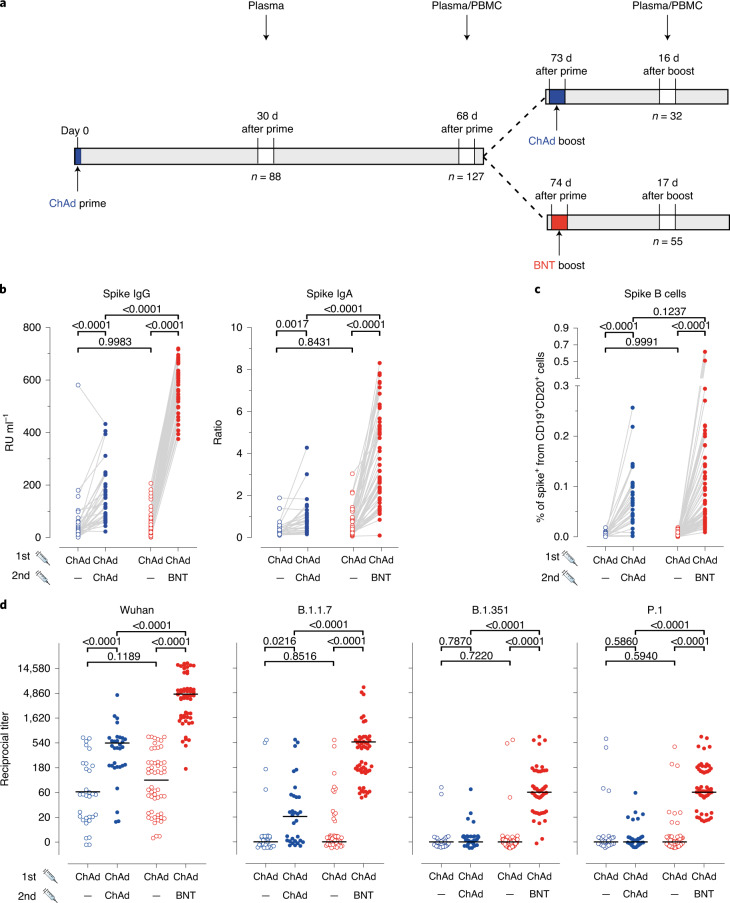
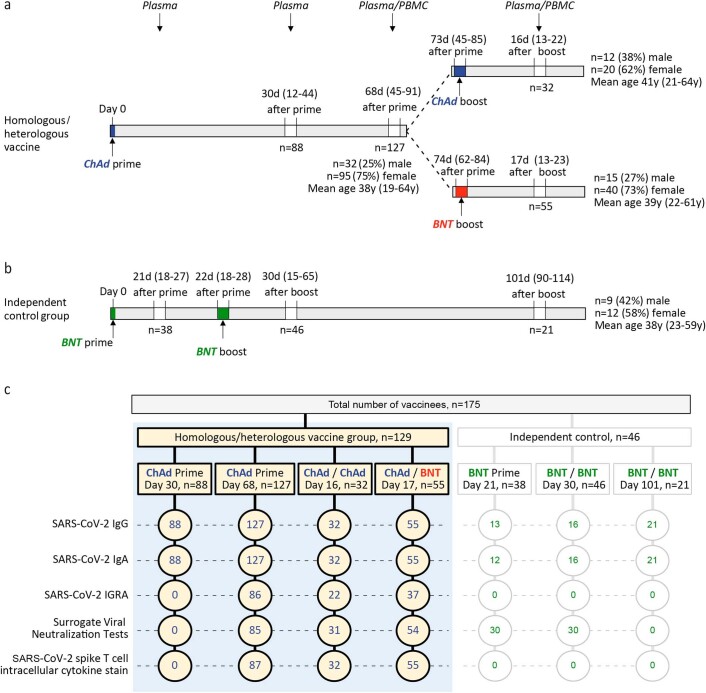
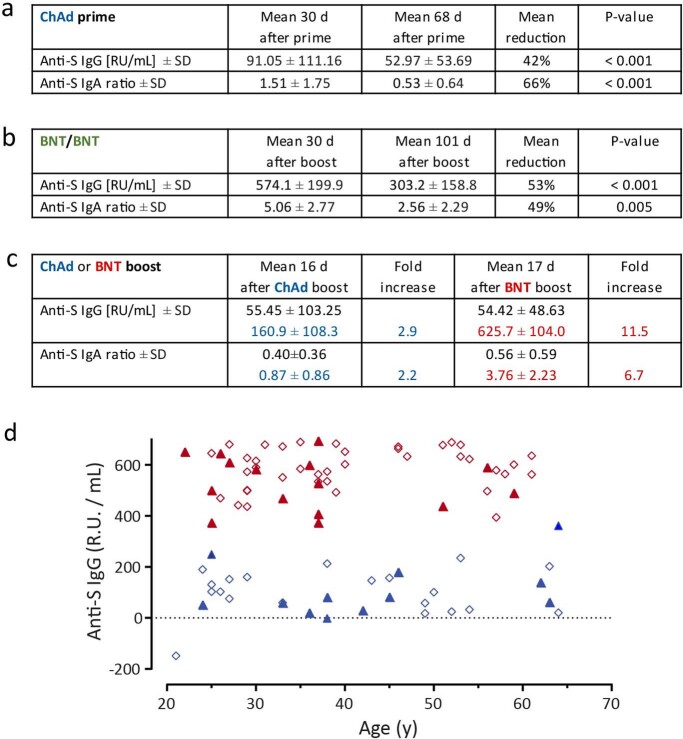
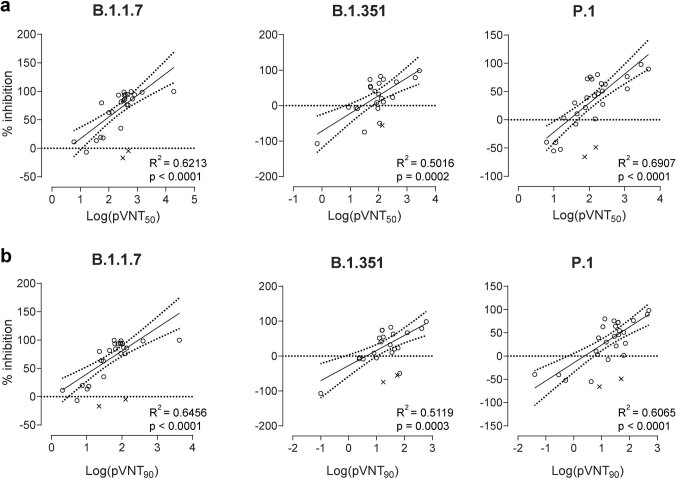
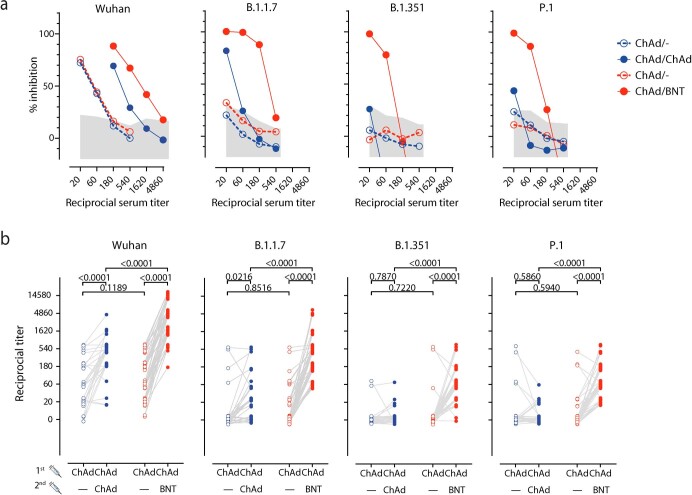
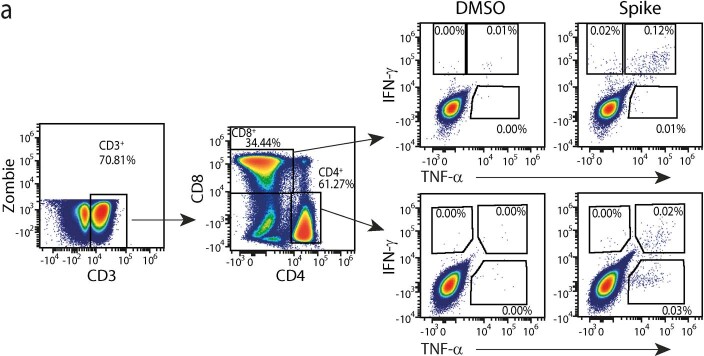
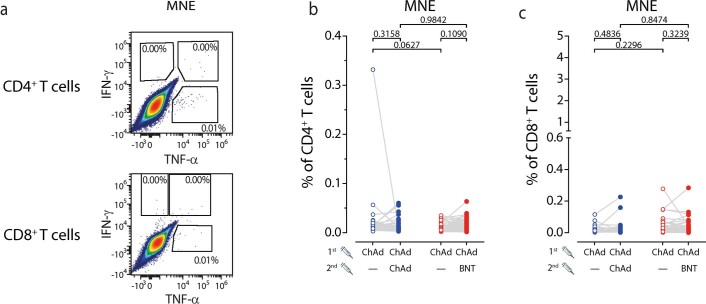
Currently approved viral vector-based and mRNA-based vaccine approaches against coronavirus disease 2019 (COVID-19) consider only homologous prime-boost vaccination. After reports of thromboembolic events, several European governments recommended using AstraZeneca's ChAdOx1-nCov-19 (ChAd) only in individuals older than 60 years, leaving millions of already ChAd-primed individuals with the decision to receive either a second shot of ChAd or a heterologous boost with mRNA-based vaccines. However, such combinations have not been tested so far. We used Hannover Medical School's COVID-19 Contact Study cohort of healthcare professionals to monitor ChAd-primed immune responses before and 3 weeks after booster with ChAd (n = 32) or BioNTech/Pfizer's BNT162b2 (n = 55). Although both vaccines boosted prime-induced immunity, BNT162b2 induced significantly higher frequencies of spike-specific CD4+ and CD8+ T cells and, in particular, high titers of neutralizing antibodies against the B.1.1.7, B.1.351 and P.1 variants of concern of severe acute respiratory syndrome coronavirus 2.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Comment in
-
A 'mix and match' approach to SARS-CoV-2 vaccination.Nat Med. 2021 Sep;27(9):1510-1511. doi: 10.1038/s41591-021-01463-x. Nat Med. 2021. PMID: 34312555 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- 80018019238/Deutsches Zentrum für Infektionsforschung (German Center for Infection Research)
- TTU 01.938/Deutsches Zentrum für Infektionsforschung (German Center for Infection Research)
- ID39087428/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 158989968/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 14-76103-184/Niedersächsische Ministerium für Wissenschaft und Kultur (Lower Saxony Ministry of Science and Culture)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
