

Comprehensive review of surgical approaches to the elbow
- PMID: 34262848
- PMCID: PMC8254122
- DOI: 10.1016/j.jcot.2021.101482
Comprehensive review of surgical approaches to the elbow
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Jul 30;20:101539. doi: 10.1016/j.jcot.2021.101539. eCollection 2021 Sep. J Clin Orthop Trauma. 2021. PMID: 34405084 Free PMC article.
Abstract
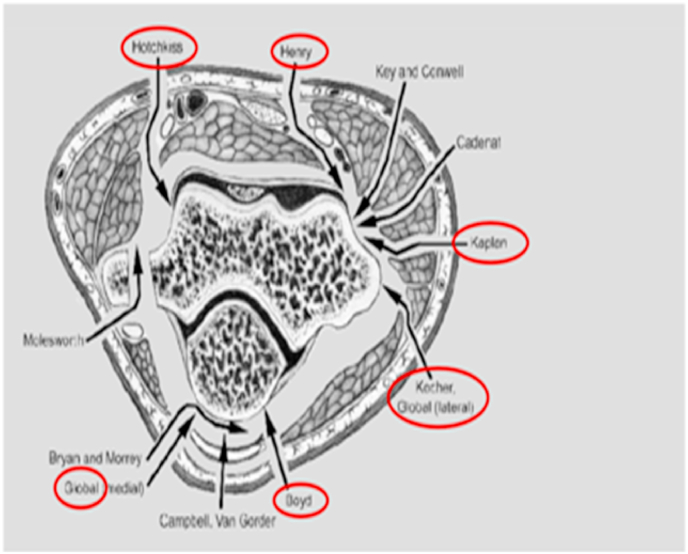
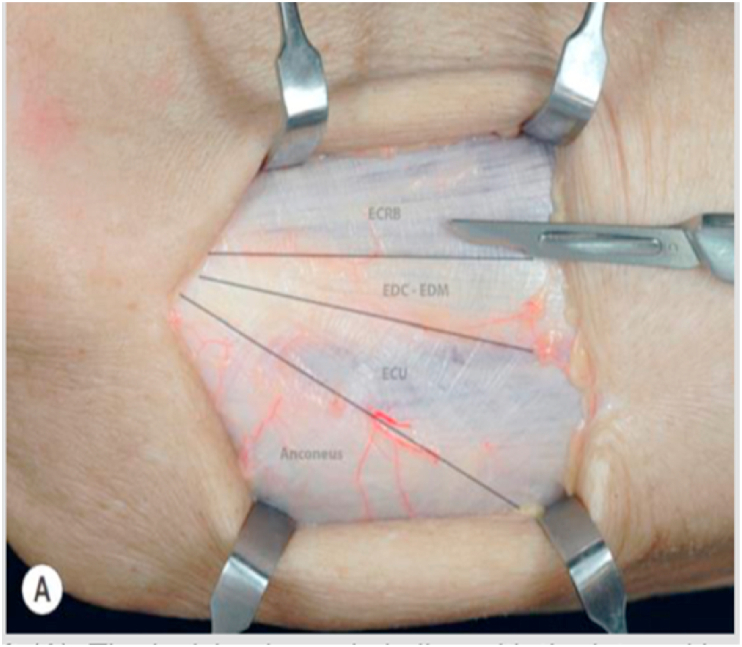
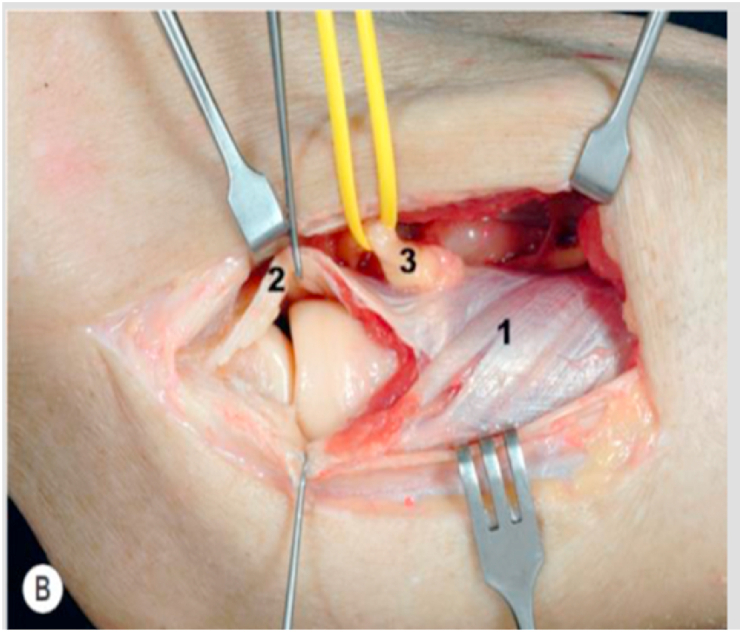
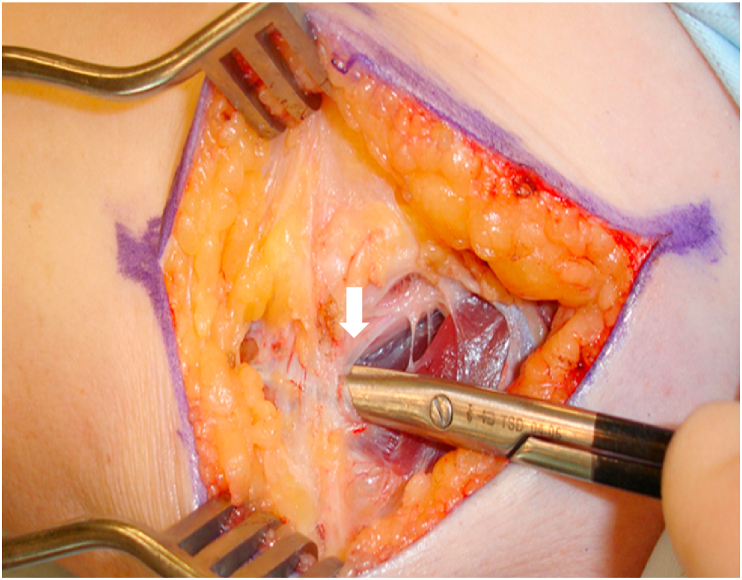
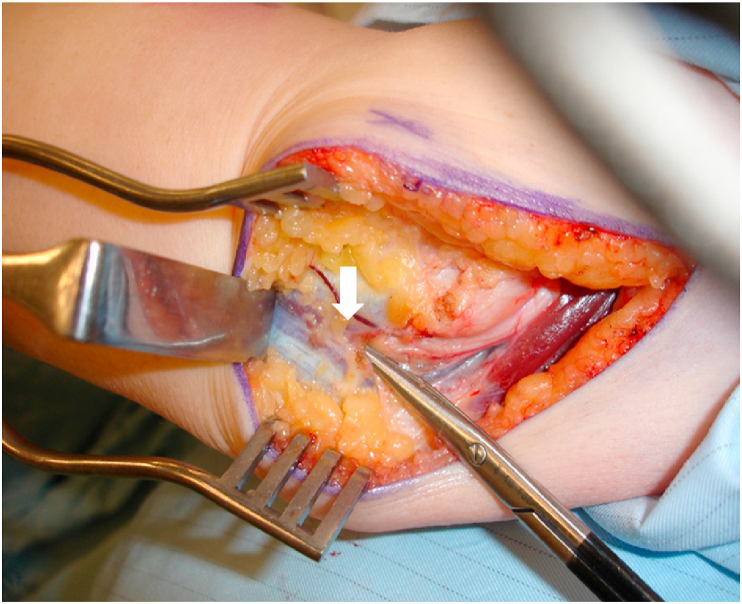
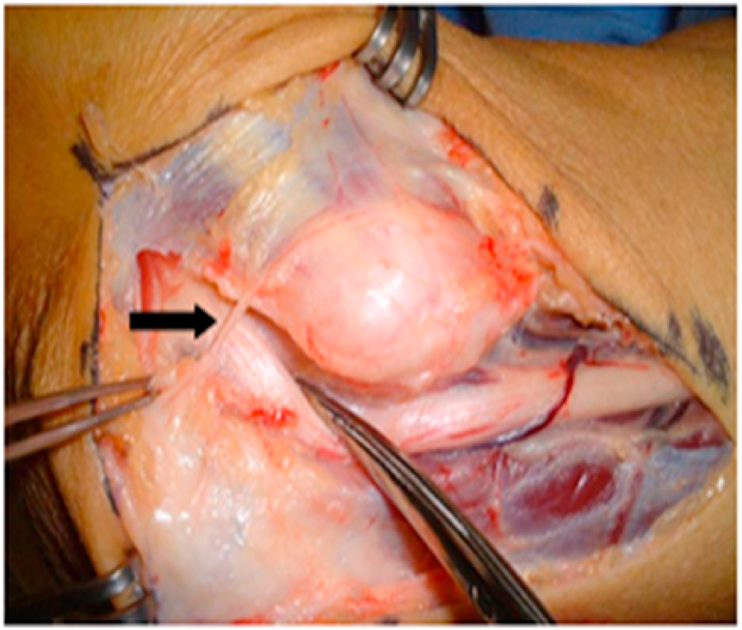
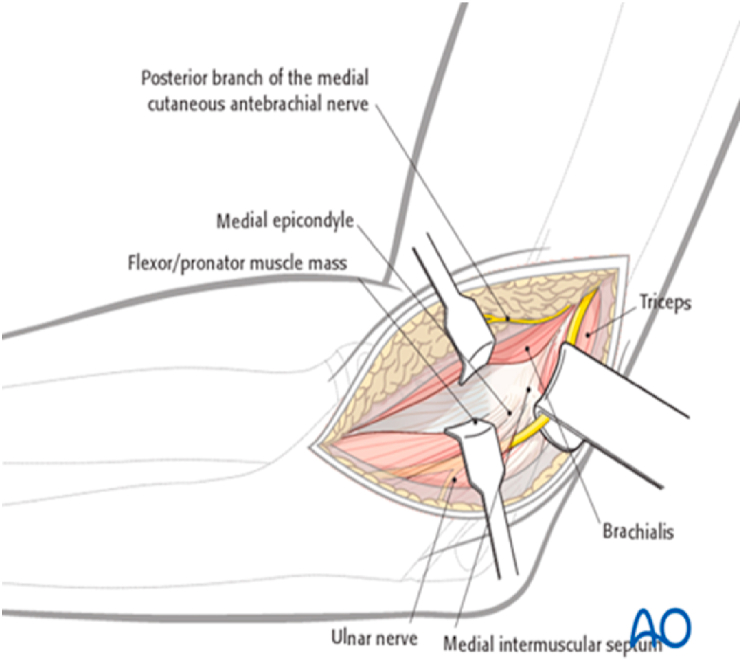
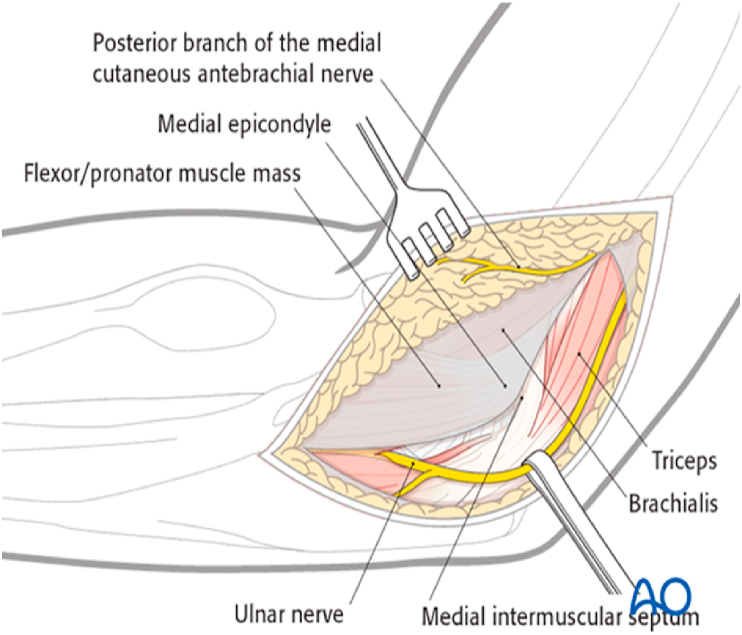
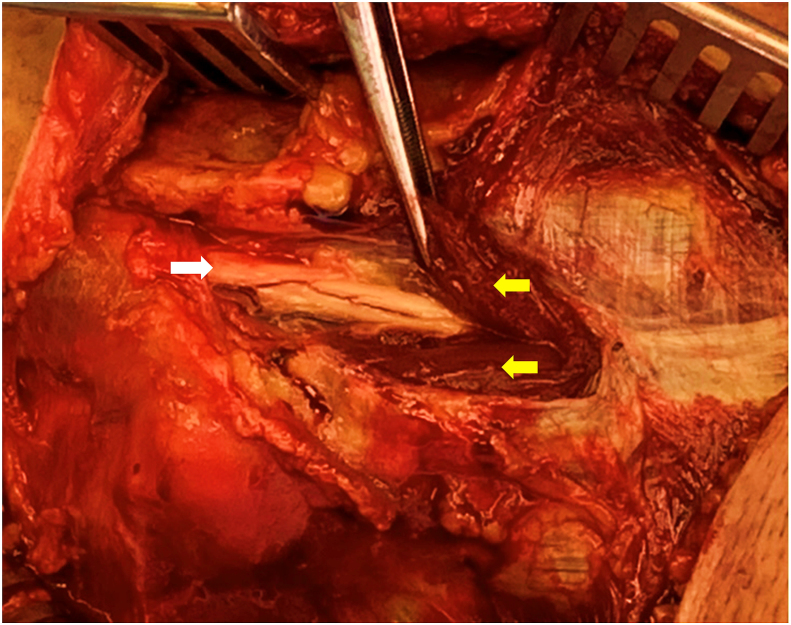
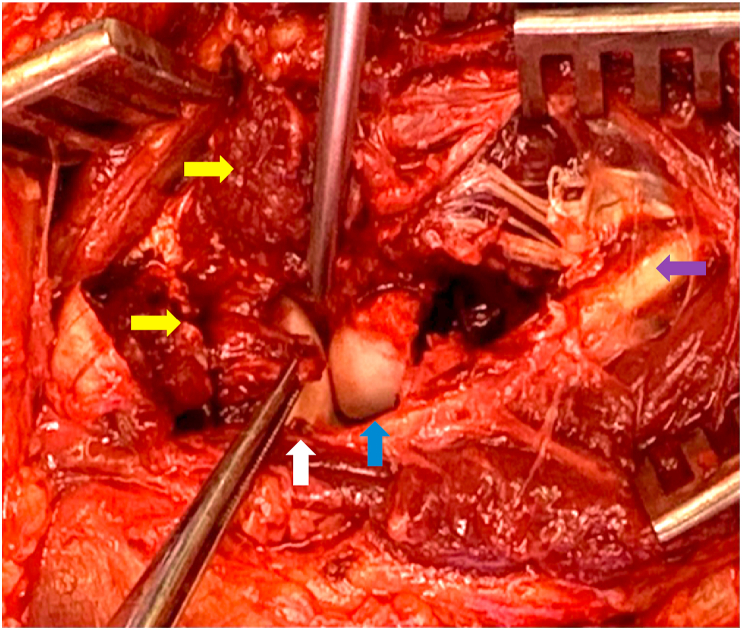
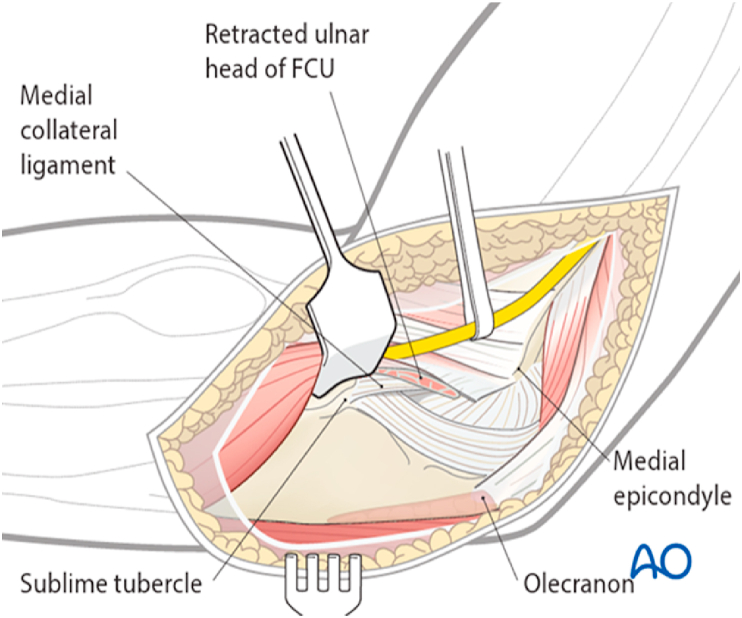
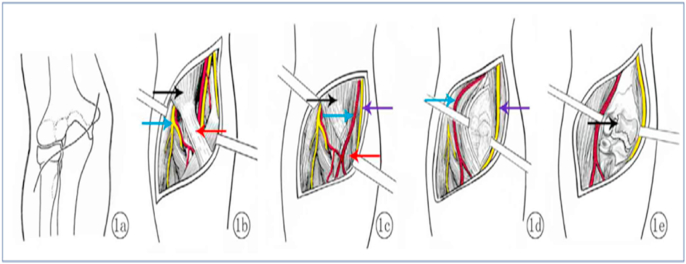
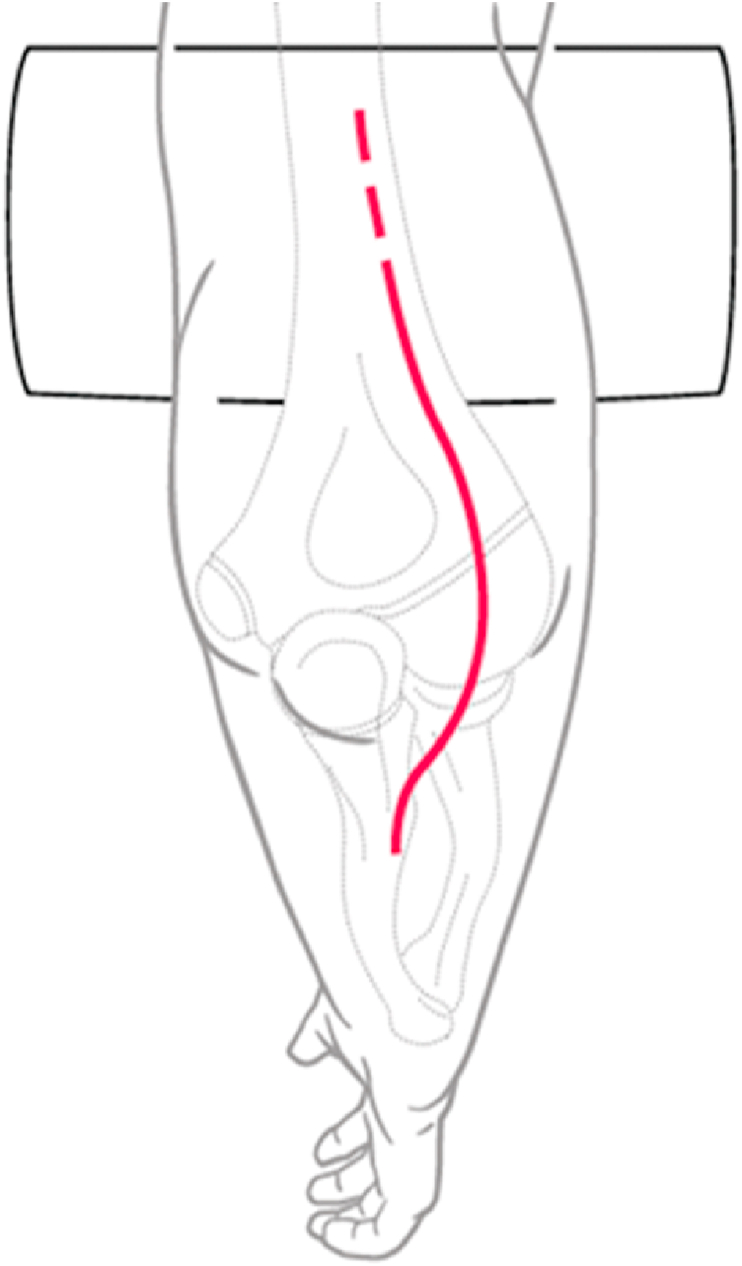
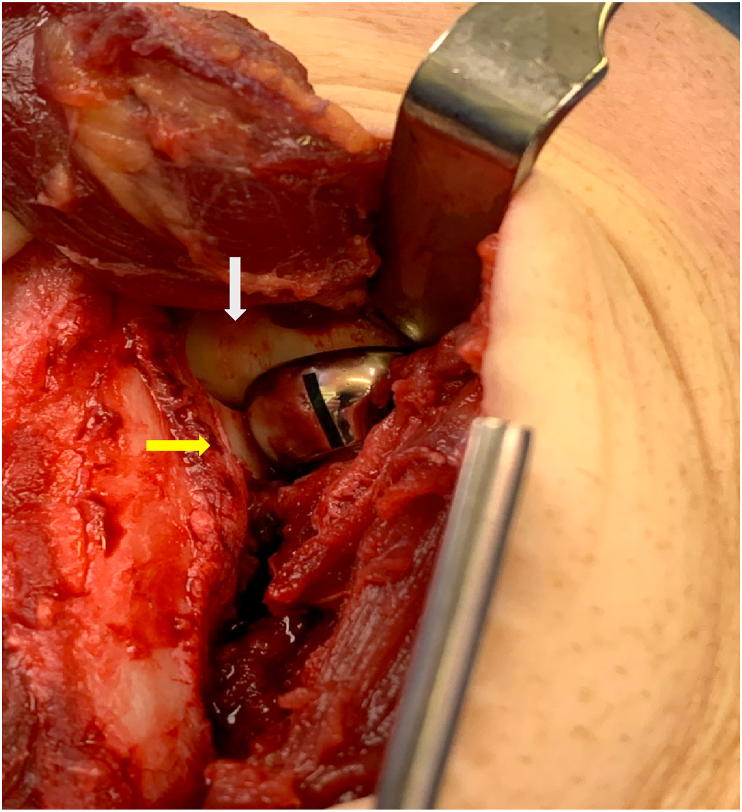
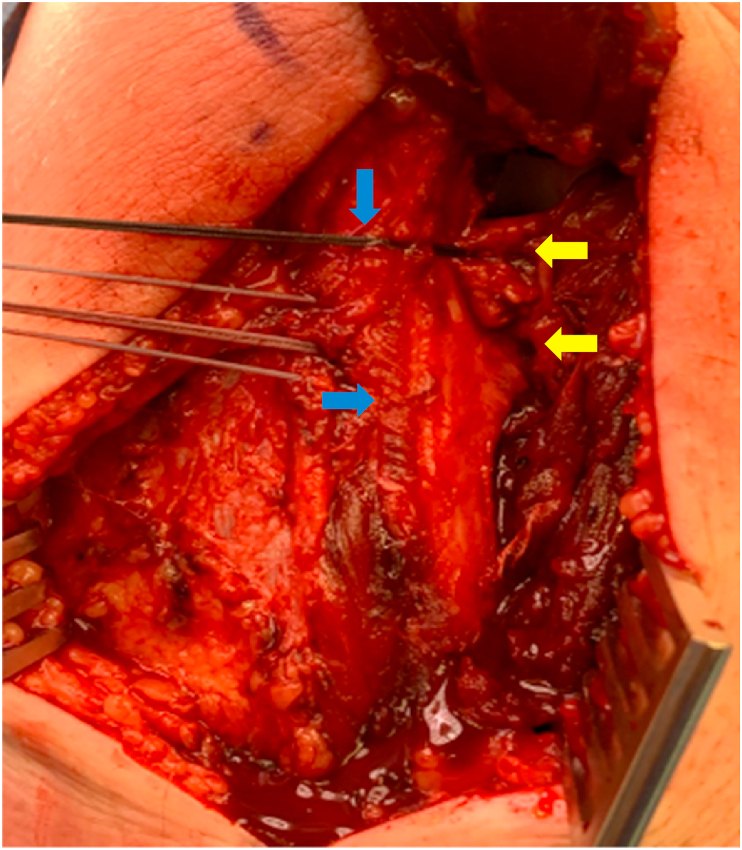
The choice of the most suitable surgical approach to the elbow forms the foundation of any successful elbow surgery. The surgical approach is based on the injury or pathology to be addressed and therefore specific anatomical details need to be considered. The surgeon must be comfortable with the bony, ligamentous and neurovascular anatomy of the elbow to consider and execute the best approach for each problem. This is an imperative to avoid iatrogenic injury. This article provides a detailed analysis, valuable technical tips, advantages and disadvantages of the most common approaches to the elbow. The lateral approaches include the Kocher, Kaplan and Extensor Digitorum Communis (EDC) Split approaches, the medial approaches include the Hotchkiss, Flexor carpi ulnaris (FCU) splitting approach, the Taylor and Scham approach. The anterior approach includes the anterior neurovascular interval approach and the posterior approaches include the Olecranon osteotomy, triceps sparing, triceps reflecting approach and finally the Boyd interval approach. The text and illustrations will provide a structured overview for the practicing surgeon.
Keywords: Anterior approach; Elbow approaches; Kaplan approach; Kocher approach; Olecranon osteotomy approach; Triceps on and triceps off approaches.
© 2021 Delhi Orthopedic Association. All rights reserved.
Figures
References
-
- William D., Hakim L., Steven R., Whitcomb P J. Objective analysis of lateral elbow exposure with the extensor digitorum communis split compared with the kocher interval. J Bone Joint Surg Am. 2014;96:387–393. - PubMed
-
- Van Leeuwen D.H., Guitton T.H., Lambers K., Ring D. Quantitative measurement of radial head fracture location. J Shoulder Elbow Surg. 2012. Aug;21(8):1023. 7Epub 2011 Nov 09. - PubMed
-
- Schimizzi A., MacLennanA, Meier K.M., Chia B., Lw3rd Catalano, Gilckel S.Z. Defining a safe zone of dissecting during the extensor digitorum communis splitting approach to the proximal radius and forearm : an anatomical study. J Hand Surg Am. 2009 Sep;34(7):125. 5. - PubMed
LinkOut - more resources
Full Text Sources