

Long-term, Prolonged-release Tacrolimus-based Immunosuppression in De Novo Liver Transplant Recipients: 5-year Prospective Follow-up of Patients in the DIAMOND Study
- PMID: 34263020
- PMCID: PMC8274734
- DOI: 10.1097/TXD.0000000000001166
Long-term, Prolonged-release Tacrolimus-based Immunosuppression in De Novo Liver Transplant Recipients: 5-year Prospective Follow-up of Patients in the DIAMOND Study
Erratum in
-
Erratum: Long-term, Prolonged-release Tacrolimus-based Immunosuppression in De Novo Liver Transplant Recipients: 5-year Prospective Follow-up of Patients in the DIAMOND Study: Erratum.Transplant Direct. 2021 Nov 15;7(12):e786. doi: 10.1097/TXD.0000000000001259. eCollection 2021 Dec. Transplant Direct. 2021. PMID: 34805488 Free PMC article.
Abstract
Background: Immunosuppression with calcineurin inhibitors (CNIs) is reportedly associated with risk of renal impairment in liver transplant recipients. It is believed that this can be mitigated by decreasing initial exposure to CNIs or delaying CNI introduction until 3-4 d posttransplantation. The ADVAGRAF studied in combination with mycophenolate mofetil and basiliximab in liver transplantation (DIAMOND) trial evaluated different administration strategies for prolonged-release tacrolimus (PR-T).
Methods: DIAMOND was a 24-wk, open-label, phase 3b trial in de novo liver transplant recipients randomized to: PR-T 0.2 mg/kg/d (Arm 1); PR-T 0.15-0.175 mg/kg/d plus basiliximab (Arm 2); or PR-T 0.2 mg/kg/d delayed until day 5 posttransplant plus basiliximab (Arm 3). In a 5-y follow-up, patients were maintained on an immunosuppressive regimen according to standard clinical practice (NCT02057484). Primary endpoint: graft survival (Kaplan-Meier analysis).
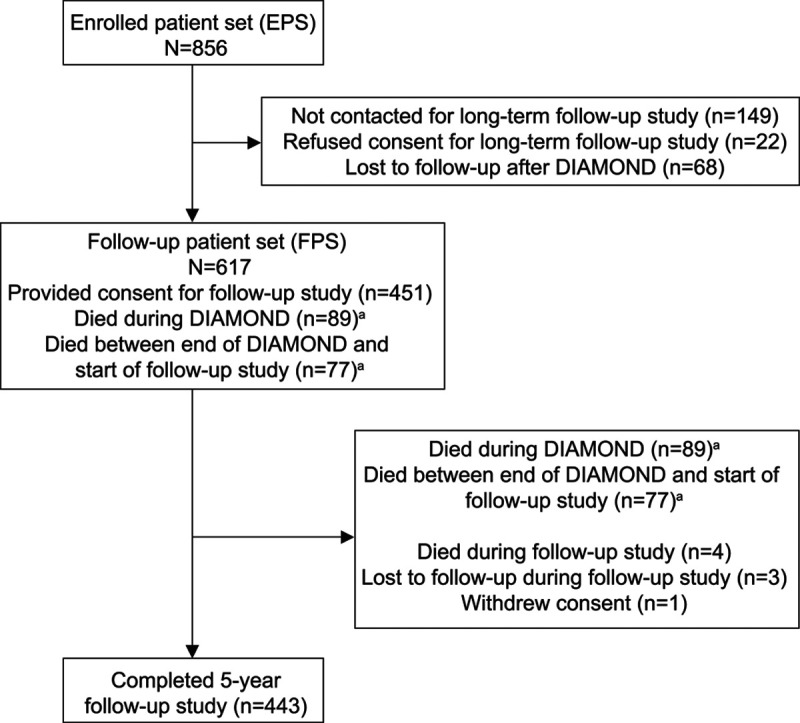
Results: Follow-up study included 856 patients. Overall graft survival was 84.6% and 73.5% at 1 and 5 y post transplant, respectively. Five-year rates for Arms 1, 2, and 3 were 74.7%, 71.5%, and 74.5%, respectively. At 5 y, death-censored graft survival in the entire cohort was 74.7%. Overall graft survival in patients remaining on PR-T for ≥30 d was 79.1%. Graft survival in patients who remained on PR-T at 5 y was 87.3%. Patient survival was 86.6% at 1 y and 76.3% at 5 y, with survival rates similar in the 3 treatment arms at 5 y. Estimated glomerular filtration rate at the end of the 24-wk initial study and 5 y posttransplant was 62.1 and 61.5 mL/min/1.73 m2, respectively, and was similar between the 3 treatment arms at 5 y. Overall, 18 (2.9%) patients had ≥1 adverse drug reaction, considered possibly related to PR-T in 6 patients.
Conclusions: In the DIAMOND study patient cohort, renal function, graft survival, and patient survival were similar between treatment arms at 5 y posttransplant.
Copyright © 2021 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
S.A., M.H., and N.U. were employees of Astellas at the time of the study. G.K. is a consultant statistician working on behalf of Astellas, and he has also received support for travel from Astellas. All authors received nonfinancial support from Astellas during the conduct of the study.
Figures



References
-
- Carrion AF, Martin P. When to refer for liver transplantation. Am J Gastroenterol. 2019; 114:7–10. - PubMed
-
- American College of Gastroenterology. Liver transplantation. 2013. Available at http://patients.gi.org/topics/liver-transplantation. Accessed October 19, 2018.
-
- Adam R, Karam V, Cailliez V, et al. ; all the other 126 contributing centers (www.eltr.org) and the European Liver and Intestine Transplant Association (ELITA). 2018 Annual Report of the European Liver Transplant Registry (ELTR) - 50-year evolution of liver transplantation. Transpl Int. 2018; 31:1293–1317. - PubMed
-
- Neuberger JM, Bechstein WO, Kuypers DR, et al. . Practical recommendations for long-term management of modifiable risks in kidney and liver transplant recipients: a guidance report and clinical checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation. 2017; 101(4S Suppl 2):S1–S56. - PubMed
-
- Wadström J, Ericzon BG, Halloran PF, et al. . Advancing transplantation: new questions, new possibilities in kidney and liver transplantation. Transplantation. 2017; 101(Suppl 2S):S1–S41. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
