

Effect of language interpretation modality on throughput and mortality for critical care patients: A retrospective observational study
- PMID: 34263246
- PMCID: PMC8253091
- DOI: 10.1002/emp2.12477
Effect of language interpretation modality on throughput and mortality for critical care patients: A retrospective observational study
Abstract
Objective: Limited data exist describing possible delays in patient transfer from the emergency department (ED) as a result of language barriers and the effects of interpretation services. We described the differences in ED length of stay (LOS) before intensive care unit (ICU) arrival and mortality based on availability of telephone or in-person interpretation services.
Methods: Using an ICU database from an urban academic tertiary care hospital, ED patients entering the ICU were divided into groups based on primary language and available interpretation services (in-person vs telephone). Non-parametric tests were used to compare ED LOS and mortality between groups.
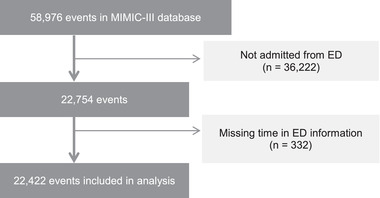
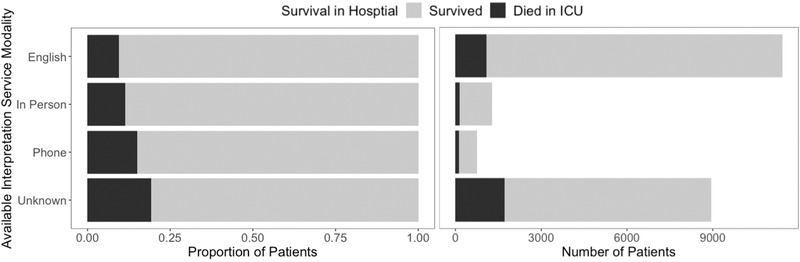
Results: Among 22,422 included encounters, English was recorded as the primary language for 51% of patients (11,427), and 9% of patients (2042) had a primary language other than English. Language was not documented for 40% of patients (8953). Among encounters with patients with non-English primary languages, in-person interpretation was available for 63% (1278) and telephone interpretation was available for 37% (764). In the English-language group, median ED LOS was 292 minutes (interquartile range [IQR], 205-412) compared with 309 minutes (IQR, 214-453) for patients speaking languages with in-person interpretation available and 327 minutes (IQR, 225-463) for patients speaking languages with telephone interpretation available. Mortality was higher among patients with telephone (15%) or in-person (11%) interpretation available compared with patients who primarily spoke English (9%).
Conclusions: Patients with primary languages other than English who were critically ill spent a median of 17 to 35 more minutes in the ED before ICU arrival and experienced higher mortality rates compared with patients who spoke English as a primary language.
Keywords: Communication barriers; Critical care; Emergency service, hospital; Health services accessibility; Language; Length of stay; Telephone.
© 2021 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Reese P. As ER wait times grow, more patients leave against medical advice. California Healthline. Published 2019. https://khn.org/news/as-er-wait-times-grow-more-patients-leave-against-m.... Accessed November 20, 2020.
-
- Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP, DELAY‐ED study group . Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477‐1483. - PubMed
-
- Wu B, Banks P, Conwell D. Disparities in emergency department wait times for acute gastrointestinal illnesses: results from the National Hospital Ambulatory Medical Care Survey, 1997–2006. Am J Gastroenterol. 2009;104:1668‐1673. - PubMed
-
- Pines JM, Russell Localio A, Hollander JE. Racial disparities in emergency department length of stay for admitted patients in the United States. Acad Emerg Med. 2009;16:403‐410. - PubMed
LinkOut - more resources
Full Text Sources
