

Stage Migration and Survival Trends in Laryngeal Cancer
- PMID: 34263369
- PMCID: PMC9013009
- DOI: 10.1245/s10434-021-10318-1
Stage Migration and Survival Trends in Laryngeal Cancer
Abstract
Background: During the last two decades, significant advancements in the treatment of laryngeal cancer have occurred. Although survival of head and neck cancer patients has improved over time, the temporal trend of laryngeal cancer survival is an area of controversy.
Methods: From 2004 to 2016, 77,527 patients who had laryngeal cancer treated with curative intent in the United States were identified in the National Cancer Database. Relative and observed survival rates were assessed for temporal trends. Multinomial logistic regression investigated the relationship between American Joint Committee on Cancer (AJCC) stage and increasing calendar year.
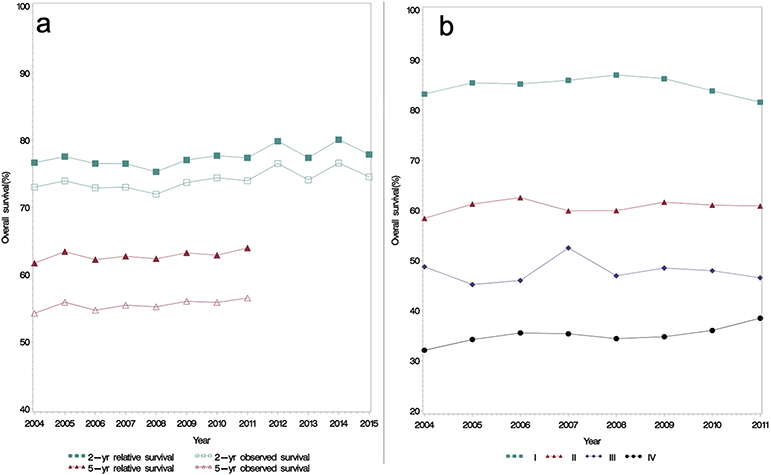
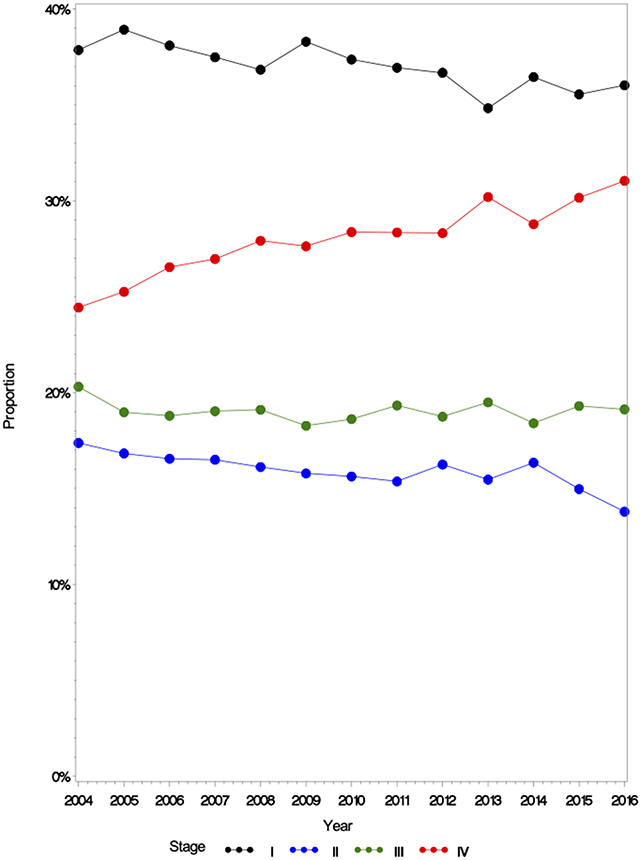
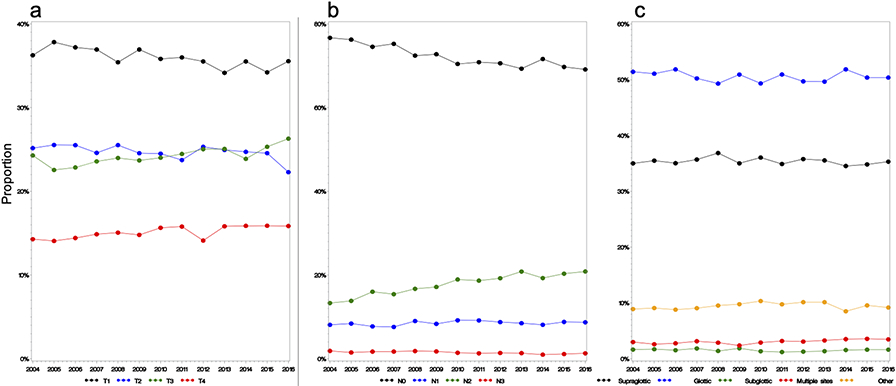
Results: No significant improvement in 2- or 5-year observed survival (OS) or relative survival (RS) was observed. The 5-year RS ranged from 61.72 to 63.97%, and the 5-year OS ranged from 54.26 to 56.52%. With each increasing year, the proportion of stage 4 disease increased, with risk for stage 4 disease at the time of diagnosis increasing 2.2% annually (adjusted odds ratio [aOR], 1.022; 95% confidence interval [CI], 1.017-1.028; p < 0.001). This increase was driven by a 4.7% yearly increase in N2 disease (aOR, 1.047; 95% CI, 1.041-1.053; p < 0.001), with an annual 1.2% increase in T3 disease (aOR, 1.012; 95% CI, 1.007-1.018; p < 0.001) and a 1.2% increase in T4 disease (aOR, 1.012; 95% CI, 1.005-1.018; p < 0.001).
Conclusion: Despite advances in the field, laryngeal cancer survival in the United States is not improving over time. This may be due to an increase in the proportion of stage 4 disease, driven primarily by increasing nodal disease. To achieve survival improvement commensurate with scientific and technologic advances, efforts should be made to diagnose and treat laryngeal cancer at earlier stages to prevent further stage migration.
© 2021. Society of Surgical Oncology.
Figures
Comment in
-
ASO Author Reflections: Stage 4 Laryngeal Cancer Rising in the United States.Ann Surg Oncol. 2021 Nov;28(12):7310. doi: 10.1245/s10434-021-10325-2. Epub 2021 Jul 15. Ann Surg Oncol. 2021. PMID: 34263370 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
