

Alpha-protein kinase 3 (ALPK3) truncating variants are a cause of autosomal dominant hypertrophic cardiomyopathy
- PMID: 34263907
- PMCID: PMC8380059
- DOI: 10.1093/eurheartj/ehab424
Alpha-protein kinase 3 (ALPK3) truncating variants are a cause of autosomal dominant hypertrophic cardiomyopathy
Abstract
Aims: The aim of this study was to determine the frequency of heterozygous truncating ALPK3 variants (ALPK3tv) in patients with hypertrophic cardiomyopathy (HCM) and confirm their pathogenicity using burden testing in independent cohorts and family co-segregation studies.
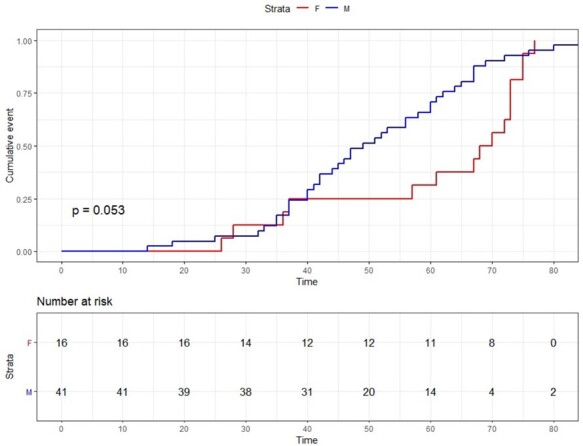
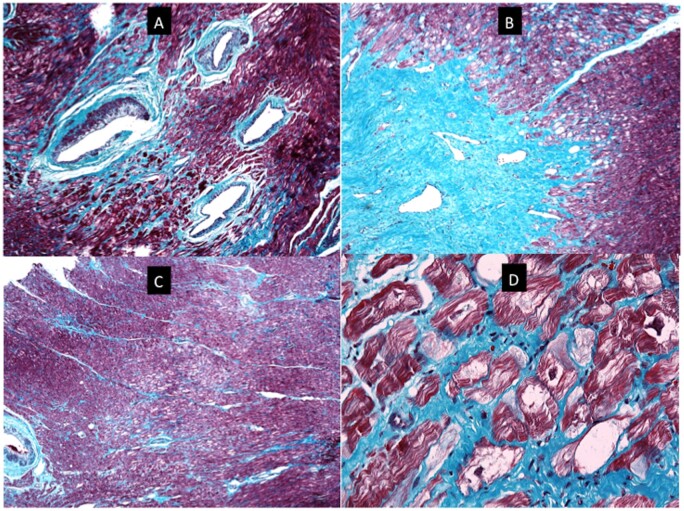
Methods and results: In a discovery cohort of 770 index patients with HCM, 12 (1.56%) were heterozygous for ALPK3tv [odds ratio(OR) 16.11, 95% confidence interval (CI) 7.94-30.02, P = 8.05e-11] compared to the Genome Aggregation Database (gnomAD) population. In a validation cohort of 2047 HCM probands, 32 (1.56%) carried heterozygous ALPK3tv (OR 16.17, 95% CI 10.31-24.87, P < 2.2e-16, compared to gnomAD). Combined logarithm of odds score in seven families with ALPK3tv was 2.99. In comparison with a cohort of genotyped patients with HCM (n = 1679) with and without pathogenic sarcomere gene variants (SP+ and SP-), ALPK3tv carriers had a higher prevalence of apical/concentric patterns of hypertrophy (60%, P < 0.001) and of a short PR interval (10%, P = 0.009). Age at diagnosis and maximum left ventricular wall thickness were similar to SP- and left ventricular systolic impairment (6%) and non-sustained ventricular tachycardia (31%) at baseline similar to SP+. After 5.3 ± 5.7 years, 4 (9%) patients with ALPK3tv died of heart failure or had cardiac transplantation (log-rank P = 0.012 vs. SP- and P = 0.425 vs. SP+). Imaging and histopathology showed extensive myocardial fibrosis and myocyte vacuolation.
Conclusions: Heterozygous ALPK3tv are pathogenic and segregate with a characteristic HCM phenotype.
Keywords: ALPK3; Genetics; Hypertrophic cardiomyopathy.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures






Comment in
-
ALPK3: a full spectrum cardiomyopathy gene?Eur Heart J. 2021 Aug 21;42(32):3074-3077. doi: 10.1093/eurheartj/ehab415. Eur Heart J. 2021. PMID: 34263911 No abstract available.
References
-
- Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2733–2779. - PubMed
-
- Ingles J, Goldstein J, Thaxton C, Caleshu C, Corty EW, Crowley SB, Dougherty K, Harrison SM, McGlaughon J, Milko LV, Morales A, Seifert BA, Strande N, Thomson K, van Tintelen JP, Wallace K, Walsh R, Wells Q, Whiffin N, Witkowski L, Semsarian C, Ware JS, Hershberger RE, Funke B. Evaluating the clinical validity of hypertrophic cardiomyopathy genes. Circ Genom Precis Med 2019;12:e002460. - PMC - PubMed
-
- Almomani R, Verhagen JM, Herkert JC, Brosens E, van Spaendonck-Zwarts KY, Asimaki A, van der Zwaag PA, Frohn-Mulder IM, Bertoli-Avella AM, Boven LG, van Slegtenhorst MA, van der Smagt JJ, van IWF, Timmer B, van Stuijvenberg M, Verdijk RM, Saffitz JE, Du Plessis FA, Michels M, Hofstra RM, Sinke RJ, van Tintelen JP, Wessels MW, Jongbloed JD, van de Laar IM. Biallelic truncating mutations in ALPK3 cause severe pediatric cardiomyopathy. J Am Coll Cardiol 2016;67:515–525. - PubMed
-
- Phelan DG, Anderson DJ, Howden SE, Wong RC, Hickey PF, Pope K, Wilson GR, Pebay A, Davis AM, Petrou S, Elefanty AG, Stanley EG, James PA, Macciocca I, Bahlo M, Cheung MM, Amor DJ, Elliott DA, Lockhart PJ. ALPK3-deficient cardiomyocytes generated from patient-derived induced pluripotent stem cells and mutant human embryonic stem cells display abnormal calcium handling and establish that ALPK3 deficiency underlies familial cardiomyopathy. Eur Heart J 2016;37:2586–2590. - PubMed
-
- Çağlayan AO, Sezer RG, Kaymakçalan H, Ulgen E, Yavuz T, Baranoski JF, Bozaykut A, Harmanci AS, Yalcin Y, Youngblood MW, Yasuno K, Bilgüvar K, Gunel M. ALPK3 gene mutation in a patient with congenital cardiomyopathy and dysmorphic features. Cold Spring Harb Mol Case Stud 2017;3:a001859. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
