

Nivolumab Plus Ipilimumab vs Nivolumab for Previously Treated Patients With Stage IV Squamous Cell Lung Cancer: The Lung-MAP S1400I Phase 3 Randomized Clinical Trial
- PMID: 34264316
- PMCID: PMC8283667
- DOI: 10.1001/jamaoncol.2021.2209
Nivolumab Plus Ipilimumab vs Nivolumab for Previously Treated Patients With Stage IV Squamous Cell Lung Cancer: The Lung-MAP S1400I Phase 3 Randomized Clinical Trial
Abstract
Importance: Nivolumab plus ipilimumab is superior to platinum-based chemotherapy in treatment-naive advanced non-small cell lung cancer (NSCLC). Nivolumab is superior to docetaxel in advanced pretreated NSCLC.
Objective: To determine whether the addition of ipilimumab to nivolumab improves survival in patients with advanced, pretreated, immunotherapy-naive squamous (Sq) NSCLC.
Design, setting, and participants: The Lung Cancer Master Protocol (Lung-MAP) S1400I phase 3, open-label randomized clinical trial was conducted from December 18, 2015, to April 23, 2018, randomizing patients in a 1:1 ratio to nivolumab alone or combined with ipilimumab. The median follow-up in surviving patients was 29.5 months. The trial was conducted through the National Clinical Trials Network and included patients with advanced immunotherapy-naive SqNSCLC and a Zubrod score of 0 (asymptomatic) to 1 (symptomatic but completely ambulatory) with disease progression after standard platinum-based chemotherapy. Randomization was stratified by sex and number of prior therapies (1 vs 2 or more). Data were analyzed from May 3, 2018, to February 1, 2021.
Interventions: Nivolumab, 3 mg/kg intravenously every 2 weeks, with or without ipilimumab, 1 mg/kg intravenously every 6 weeks, until disease progression or intolerable toxic effects.
Main outcomes and measures: The primary end point was overall survival (OS). Secondary end points included investigator-assessed progression-free survival (IA-PFS) and response per Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, version 1.1.
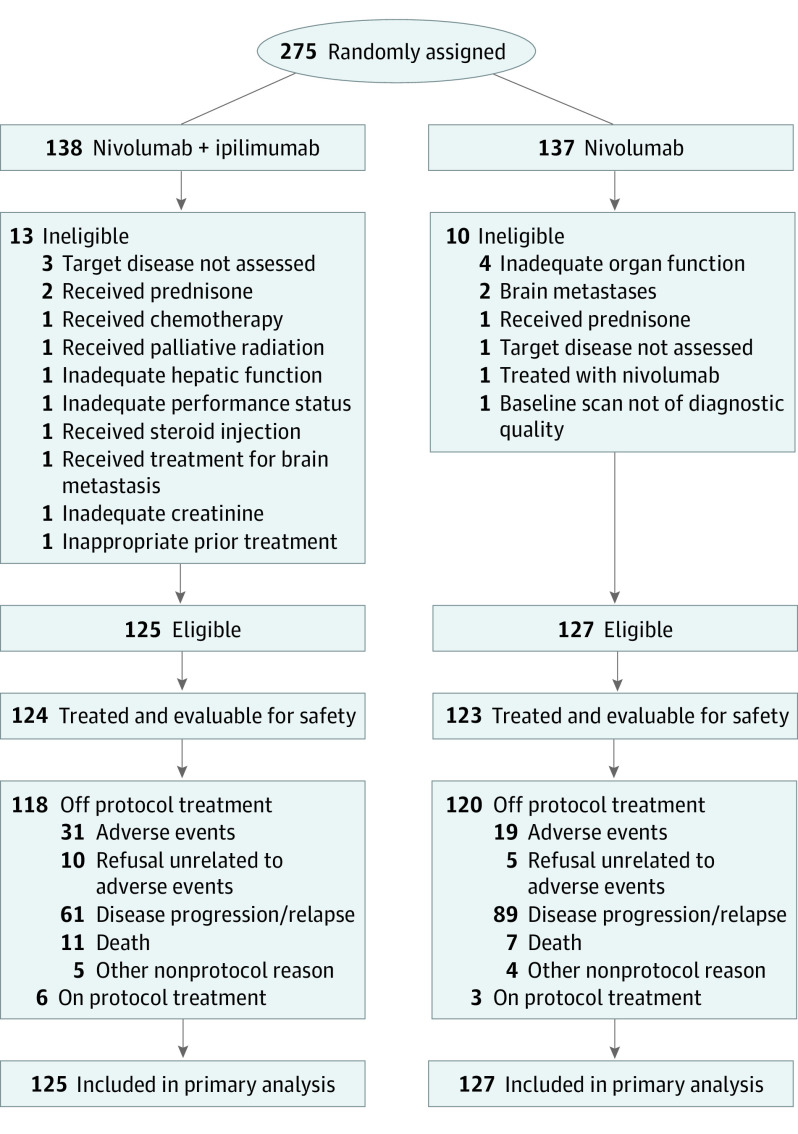
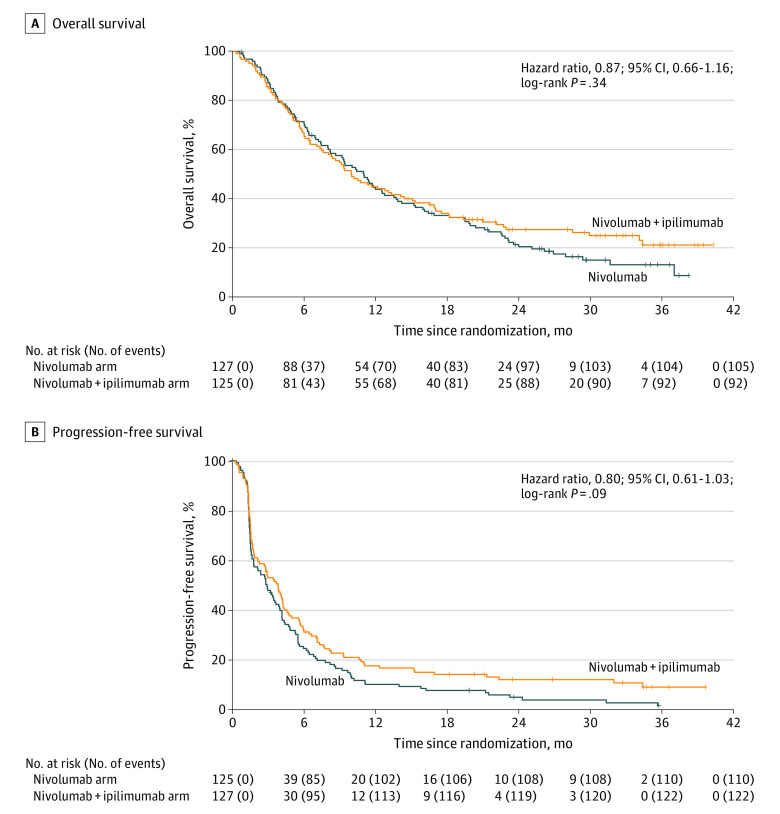
Results: Of 275 enrolled patients, 252 (mean age, 67.5 years [range 41.8-90.3 years]; 169 men [67%]; 206 White patients [82%]) were deemed eligible (125 randomized to nivolumab/ipilimumab and 127 to nivolumab). The study was closed for futility at a planned interim analysis. Overall survival was not significantly different between the groups (hazard ratio [HR], 0.87; 95% CI, 0.66-1.16; P = .34). Median survival was 10 months (95% CI, 8.0-14.4 months) in the nivolumab/ipilimumab group and 11 months (95% CI, 8.6-13.7 months) in the nivolumab group. The IA-PFS HR was 0.80 (95% CI, 0.61-1.03; P = .09); median IA-PFS was 3.8 months (95% CI, 2.7-4.4 months) in the nivolumab/ipilimumab group and 2.9 months (95% CI, 1.8-4.0 months) in the nivolumab alone group. Response rates were 18% (95% CI, 12%-25%) with nivolumab/ipilimumab and 17% (95% CI, 10%-23%) with nivolumab. Median response duration was 28.4 months (95% CI, 4.9 months to not reached) with nivolumab/ipilimumab and 9.7 months with nivolumab (95% CI, 4.2-23.1 months). Grade 3 or higher treatment-related adverse events occurred in 49 of 124 patients (39.5%) who received nivolumab/ipilimumab and in 41 of 123 (33.3%) who received nivolumab alone. Toxic effects led to discontinuation in 31 of 124 patients (25%) on nivolumab/ipilimumab and in 19 of 123 (15%) on nivolumab.
Conclusions and relevance: In this phase 3 randomized clinical trial, ipilimumab added to nivolumab did not improve outcomes in patients with advanced, pretreated, immune checkpoint inhibitor-naive SqNSCLC.
Trial registration: ClinicalTrials.gov Identifier: NCT02785952.
Conflict of interest statement
Figures
Comment in
-
Nivolumab Plus Ipilimumab for Previously Treated Stage IV Squamous Cell Lung Cancer-Reply.JAMA Oncol. 2022 Apr 1;8(4):1. doi: 10.1001/jamaoncol.2021.7790. JAMA Oncol. 2022. PMID: 35142793 No abstract available.
-
Nivolumab Plus Ipilimumab for Previously Treated Stage IV Squamous Cell Lung Cancer.JAMA Oncol. 2022 Apr 1;8(4):642. doi: 10.1001/jamaoncol.2021.7787. JAMA Oncol. 2022. PMID: 35142795 No abstract available.
-
Nivolumab Plus Ipilimumab for Previously Treated Stage IV Squamous Cell Lung Cancer.JAMA Oncol. 2022 Apr 1;8(4):641-642. doi: 10.1001/jamaoncol.2021.7784. JAMA Oncol. 2022. PMID: 35142796 No abstract available.
References
-
- Rittmeyer A, Barlesi F, Waterkamp D, et al. ; OAK Study Group . Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255-265. doi:10.1016/S0140-6736(16)32517-X - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
