

A pragmatic evidence-based approach to post-mortem perinatal imaging
- PMID: 34264420
- PMCID: PMC8282801
- DOI: 10.1186/s13244-021-01042-1
A pragmatic evidence-based approach to post-mortem perinatal imaging
Abstract
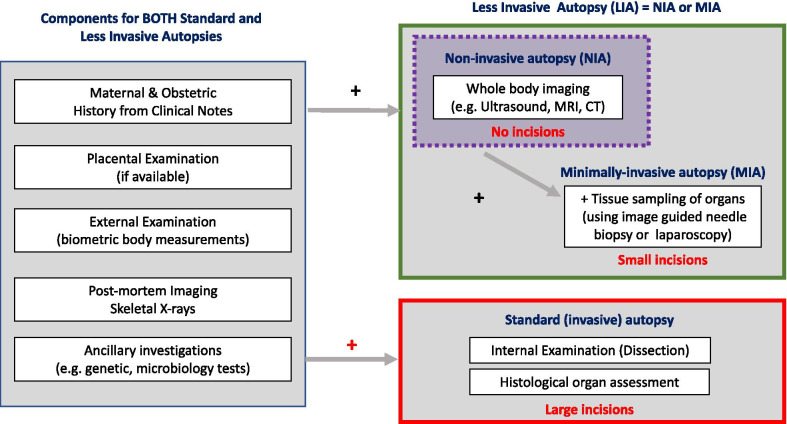
Post-mortem imaging has a high acceptance rate amongst parents and healthcare professionals as a non-invasive method for investigating perinatal deaths. Previously viewed as a 'niche' subspecialty, it is becoming increasingly requested, with general radiologists now more frequently asked to oversee and advise on appropriate imaging protocols. Much of the current literature to date has focussed on diagnostic accuracy and clinical experiences of individual centres and their imaging techniques (e.g. post-mortem CT, MRI, ultrasound and micro-CT), and pragmatic, evidence-based guidance for how to approach such referrals in real-world practice is lacking. In this review, we summarise the latest research and provide an approach and flowchart to aid decision-making for perinatal post-mortem imaging. We highlight key aspects of the maternal and antenatal history that radiologists should consider when protocolling studies (e.g. antenatal imaging findings and history), and emphasise important factors that could impact the diagnostic quality of post-mortem imaging examinations (e.g. post-mortem weight and time interval). Considerations regarding when ancillary post-mortem image-guided biopsy tests are beneficial are also addressed, and we provide key references for imaging protocols for a variety of cross-sectional imaging modalities.
Keywords: Autopsy; Diagnostic imaging; Foetus; Pregnancy loss; Radiology.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
