

Progressive exercise compared with best practice advice, with or without corticosteroid injection, for the treatment of patients with rotator cuff disorders (GRASP): a multicentre, pragmatic, 2 × 2 factorial, randomised controlled trial
- PMID: 34265255
- PMCID: PMC8343092
- DOI: 10.1016/S0140-6736(21)00846-1
Progressive exercise compared with best practice advice, with or without corticosteroid injection, for the treatment of patients with rotator cuff disorders (GRASP): a multicentre, pragmatic, 2 × 2 factorial, randomised controlled trial
Abstract
Background: Corticosteroid injections and physiotherapy exercise programmes are commonly used to treat rotator cuff disorders but the treatments' effectiveness is uncertain. We aimed to compare the clinical effectiveness and cost-effectiveness of a progressive exercise programme with a single session of best practice physiotherapy advice, with or without corticosteroid injection, in adults with a rotator cuff disorder.
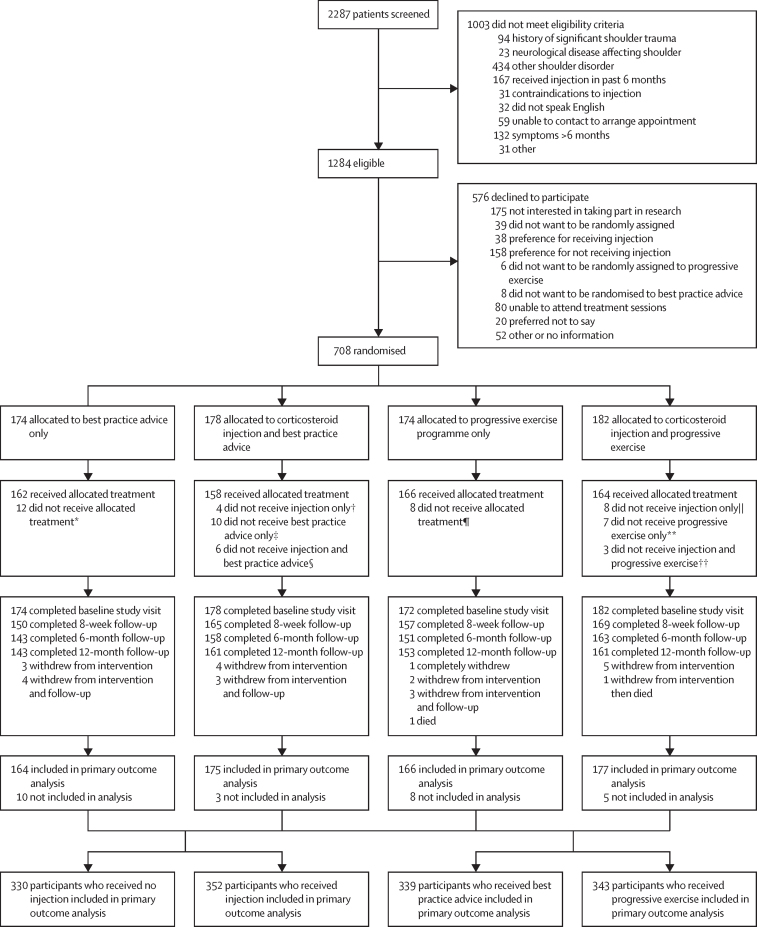
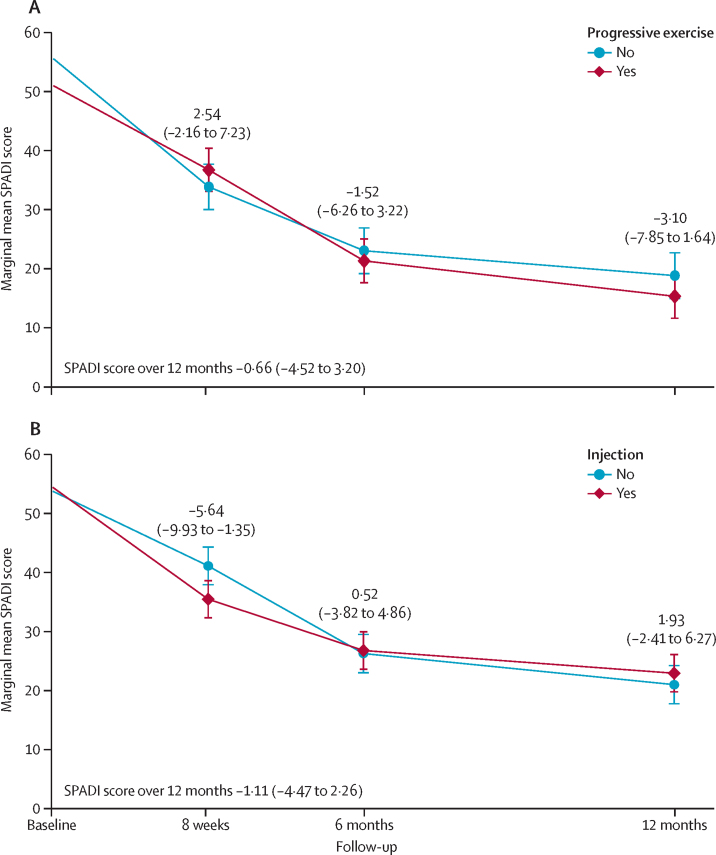
Methods: In this pragmatic, multicentre, superiority, randomised controlled trial (2 × 2 factorial), we recruited patients from 20 UK National Health Service trusts. We included patients aged 18 years or older with a rotator cuff disorder (new episode within the past 6 months). Patients were excluded if they had a history of significant shoulder trauma (eg, dislocation, fracture, or full-thickness tear requiring surgery), neurological disease affecting the shoulder, other shoulder conditions (eg, inflammatory arthritis, frozen shoulder, or glenohumeral joint instability), received corticosteroid injection or physiotherapy for shoulder pain in the past 6 months, or were being considered for surgery. Patients were randomly assigned (centralised computer-generated system, 1:1:1:1) to progressive exercise (≤6 sessions), best practice advice (one session), corticosteroid injection then progressive exercise, or corticosteroid injection then best practice advice. The primary outcome was the Shoulder Pain and Disability Index (SPADI) score over 12 months, analysed on an intention-to-treat basis (statistical significance set at 1%). The trial was registered with the International Standard Randomised Controlled Trial Register, ISRCTN16539266, and EuDRACT, 2016-002991-28.
Findings: Between March 10, 2017, and May 2, 2019, we screened 2287 patients. 708 patients were randomly assigned to progressive exercise (n=174), best practice advice (n=174), corticosteroid injection then progressive exercise (n=182), or corticosteroid injection then best practice advice (n=178). Over 12 months, SPADI data were available for 166 (95%) patients in the progressive exercise group, 164 (94%) in the best practice advice group, 177 (97%) in the corticosteroid injection then progressive exercise group, and 175 (98%) in the corticosteroid injection then best practice advice group. We found no evidence of a difference in SPADI score between progressive exercise and best practice advice when analysed over 12 months (adjusted mean difference -0·66 [99% CI -4·52 to 3·20]). We also found no evidence of a difference between corticosteroid injection compared with no injection when analysed over 12 months (-1·11 [-4·47 to 2·26]). No serious adverse events were reported.
Interpretation: Progressive exercise was not superior to a best practice advice session with a physiotherapist in improving shoulder pain and function. Subacromial corticosteroid injection provided no long-term benefit in patients with rotator cuff disorders.
Funding: UK National Institute for Health Research Technology Assessment Programme.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests SH is a member of the UK National Institute for Health Research (NIHR) Health Technology Assessment (HTA) Clinical Evaluation and Trials Committee (Nov 1, 2018, to Nov 30, 2022). DJK holds an NIHR postdoctoral fellowship. IRM holds an NIHR pre-doctoral fellowship. SJD reports grants from the NIHR HTA programme during the conduct of the study. HD is partly funded by an NIHR senior research fellowship through the Biomedical Research Centre, Oxford, UK. AC is a member of the UK Research and Innovation/Medical Research Council Developmental Pathway Funding Scheme panel. He was chief investigator of the NIHR HTA UK Rotator Cuff Surgery (UKCUFF) trial and the CSAW trial. He is a consultant to the Novartis musculoskeletal board. He is chief investigator of an NIHR i4i trial of a novel electrospun patch and of a Wellcome Trust-funded trial of a novel electrospun suture in rotator cuff repair surgery. He was director of the NIHR Musculoskeletal British Research Unit from 2008 to 2017 and is musculoskeletal theme lead for the NIHR Oxford comprehensive British Research Centre. ZH reports grants from the NIHR HTA programme during the conduct of the study and is paid personal fees by various health-care trusts and individuals to train health-care professionals in cognitive behavioural approaches, outside the submitted work. AJ is a council member of the British Shoulder and Elbow Society. She is co-applicant for the NIHR HTA (Partial Rotator Cuff Tear Repair (PROCURE) trial. CL is chair of the Chartered Society of Physiotherapy scientific panel. He is chief investigator of the NIHR post-doctoral fellowship-funded Surgery versus PhysiothErapist-leD exercise (SPeEDy) study. He was previously lead researcher for the NIHR Research for Patient Benefit funded Rehabilitation Following Rotator Cuff Repair (RaCeR) study and chief investigator for the NIHR doctoral fellowship-funded SELF (a self-managed single exercise programme versus usual physiotherapy treatment for rotator cuff tendinopathy) study. SEL reports grants from the NIHR HTA programme during the conduct of the study and was a member of the following boards: HTA Additional Capacity Funding Board 2012–15; HTA Clinical Trials Board 2010–15; HTA End of Life Care and Add on Studies 2015–15; HTA Funding Boards Policy Group (formerly CSG) 2010–15; HTA Maternal, Neonatal and Child Health Methods Group 2013–15; HTA post-board funding teleconference (Prioritisation Group members to attend) 2010–15; HTA Primary Care Themed Call board 2013–14; HTA Prioritisation Group 2010–15; and NIHR Clinical Trials Unit Standing Advisory Committee 2012–16. All other authors declare no completing interests.
Figures
Comment in
-
Optimising treatment for patients with rotator cuff disorders.Lancet. 2021 Jul 31;398(10298):369-370. doi: 10.1016/S0140-6736(21)00987-9. Epub 2021 Jul 12. Lancet. 2021. PMID: 34265254 No abstract available.
-
In rotator cuff disorder, progressive exercise vs. physiotherapy advice, with or without corticosteroid injection, did not differ at 12 mo.Ann Intern Med. 2021 Dec;174(12):JC137. doi: 10.7326/ACPJ202112210-137. Epub 2021 Dec 7. Ann Intern Med. 2021. PMID: 34871052
-
Critically appraised paper: Progressive exercise is not superior to best practice advice, and steroid injection is not superior to no injection, for rotator cuff disorders [synopsis].J Physiother. 2022 Jan;68(1):71. doi: 10.1016/j.jphys.2021.11.005. Epub 2021 Dec 8. J Physiother. 2022. PMID: 34895877 No abstract available.
-
Critically appraised paper: Progressive exercise is not superior to best practice advice, and steroid injection is not superior to no injection, for rotator cuff disorders [commentary].J Physiother. 2022 Jan;68(1):71. doi: 10.1016/j.jphys.2021.11.006. Epub 2021 Dec 8. J Physiother. 2022. PMID: 34895878 No abstract available.
References
-
- Linsell L, Dawson J, Zondervan K. Prevalence and incidence of adults consulting for shoulder conditions in UK primary care; patterns of diagnosis and referral. Rheumatology. 2006;45:215–221. - PubMed
-
- British Elbow and Shoulder Society. British Orthopaedic Association. Royal College of Surgeons Commissioning guide: subacromial shoulder pain. 2014. https://www.rcseng.ac.uk/library-and-publications/rcs-publications/docs/...
-
- Hanratty CE, McVeigh JG, Kerr DP. The effectiveness of physiotherapy exercises in subacromial impingement syndrome: a systematic review and meta-analysis. Semin Arthritis Rheum. 2012;42:297–316. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
