

Prediction of Outcome and Endovascular Treatment Benefit: Validation and Update of the MR PREDICTS Decision Tool
- PMID: 34266308
- PMCID: PMC8378416
- DOI: 10.1161/STROKEAHA.120.032935
Prediction of Outcome and Endovascular Treatment Benefit: Validation and Update of the MR PREDICTS Decision Tool
Abstract
Background and purpose: Benefit of early endovascular treatment (EVT) for ischemic stroke varies considerably among patients. The MR PREDICTS decision tool, derived from MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands), predicts outcome and treatment benefit based on baseline characteristics. Our aim was to externally validate and update MR PREDICTS with data from international trials and daily clinical practice.
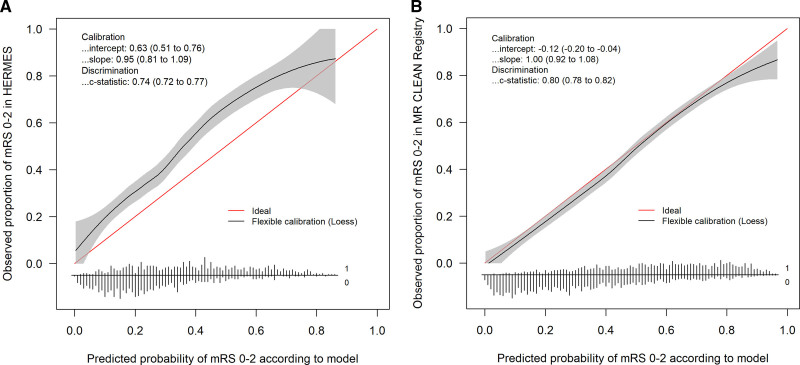
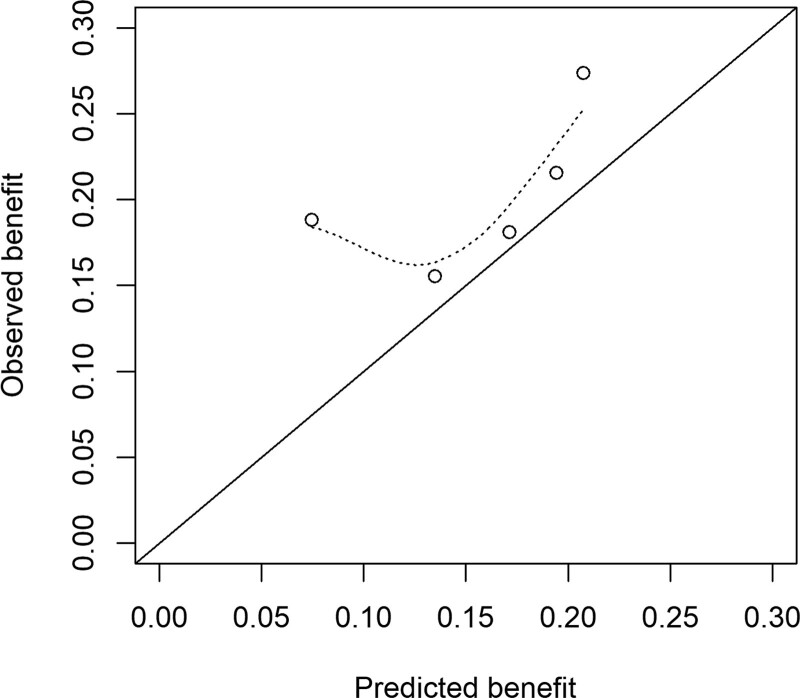
Methods: We used individual patient data from 6 randomized controlled trials within the HERMES (Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials) collaboration to validate the original model. Then, we updated the model and performed a second validation with data from the observational MR CLEAN Registry. Primary outcome was functional independence (defined as modified Rankin Scale score 0–2) 3 months after stroke. Treatment benefit was defined as the difference between the probability of functional independence with and without EVT. Discriminative performance was evaluated using a concordance (C) statistic.
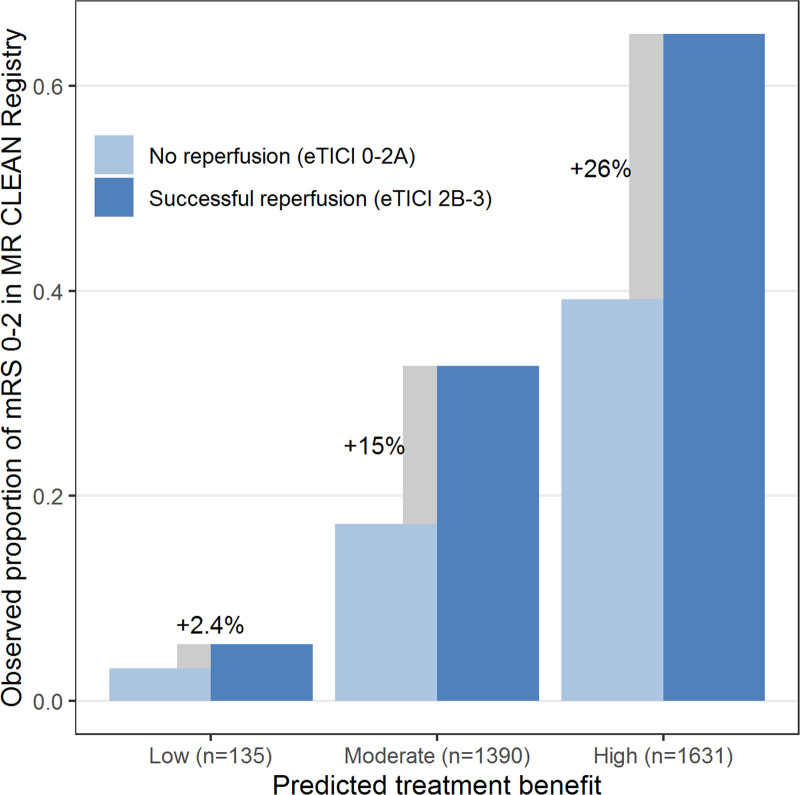
Results: We included 1242 patients from HERMES (633 assigned to EVT, 609 assigned to control) and 3156 patients from the MR CLEAN Registry (all of whom underwent EVT within 6.5 hours). The C-statistic for functional independence was 0.74 (95% CI, 0.72–0.77) in HERMES and, after model updating, 0.80 (0.78–0.82) in the Registry. Median predicted treatment benefit of routinely treated patients (Registry) was 10.3% (interquartile range, 5.8%–14.4%). Patients with low (<1%) predicted treatment benefit (n=135/3156 [4.3%]) had low rates of functional independence, irrespective of reperfusion status, suggesting potential absence of treatment benefit. The updated model was made available online for clinicians and researchers at www.mrpredicts.com.
Conclusions: Because of the substantial treatment effect and small potential harm of EVT, most patients arriving within 6 hours at an endovascular-capable center should be treated regardless of their clinical characteristics. MR PREDICTS can be used to support clinical judgement when there is uncertainty about the treatment indication, when resources are limited, or before a patient is to be transferred to an endovascular-capable center.
Keywords: ischemic stroke; registry; reperfusion; thrombectomy; uncertainty.
Figures
References
-
- Mulder MJ, Venema E, Roozenbeek B, Broderick JP, Yeatts SD, Khatri P, Berkhemer OA, Roos YB, Majoie CB, van Oostenbrugge RJ, et al. . Towards personalised intra-arterial treatment of patients with acute ischaemic stroke: A study protocol for development and validation of a clinical decision aid. BMJ Open. 2017;7:e013699. - PMC - PubMed
-
- Venema E, Mulder M, Roozenbeek B, Broderick JP, Yeatts SD, Khatri P, Berkhemer OA, Emmer BJ, Roos Y, Majoie C, et al. . Selection of patients for intra-arterial treatment for acute ischaemic stroke: Development and validation of a clinical decision tool in two randomised trials. BMJ. 2017;357:j1710. - PMC - PubMed
-
- Rothwell PM. Treating Individuals: From Randomised Trials to Personalised Medicine. 2007. Elsevier
