

The Coronary Artery Risk Development In Young Adults (CARDIA) Study: JACC Focus Seminar 8/8
- PMID: 34266580
- PMCID: PMC8285563
- DOI: 10.1016/j.jacc.2021.05.022
The Coronary Artery Risk Development In Young Adults (CARDIA) Study: JACC Focus Seminar 8/8
Abstract
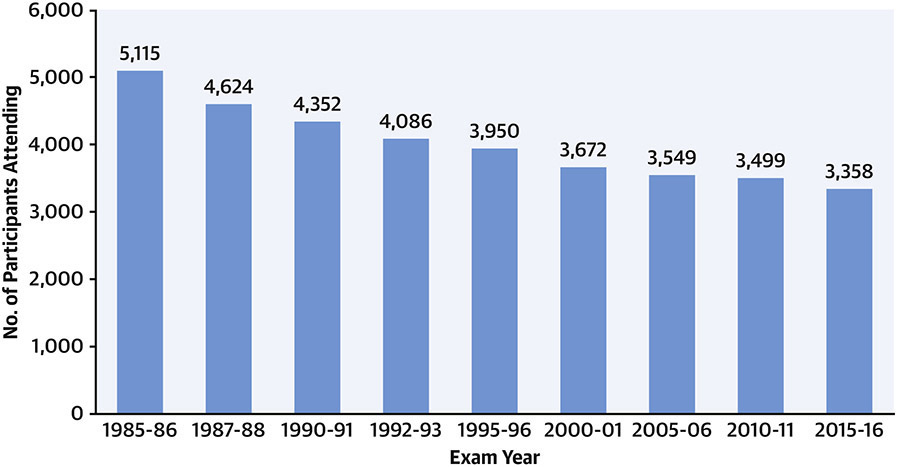
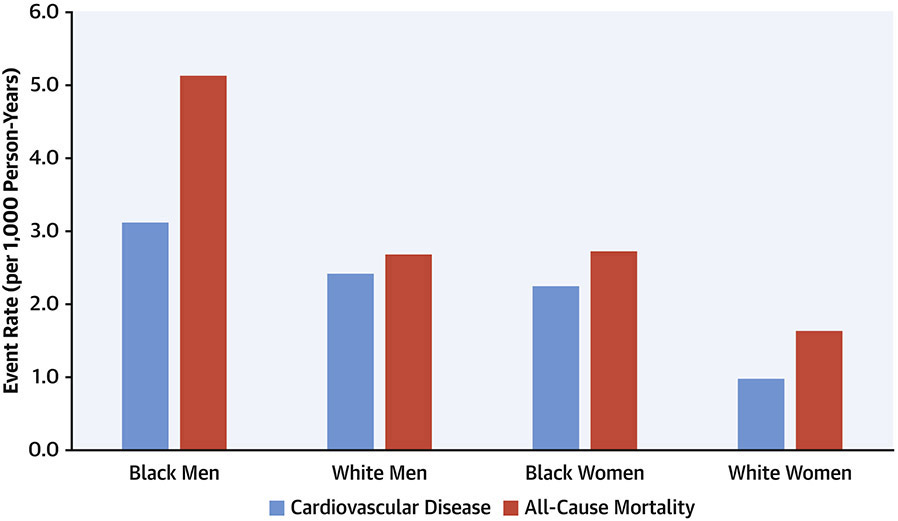
The CARDIA (Coronary Artery Risk Development in Young Adults) study began in 1985 to 1986 with enrollment of 5,115 Black or White men and women ages 18 to 30 years from 4 US communities. Over 35 years, CARDIA has contributed fundamentally to our understanding of the contemporary epidemiology and life course of cardiovascular health and disease, as well as pulmonary, renal, neurological, and other manifestations of aging. CARDIA has established associations between the neighborhood environment and the evolution of lifestyle behaviors with biological risk factors, subclinical disease, and early clinical events. CARDIA has also identified the nature and major determinants of Black-White differences in the development of cardiovascular risk. CARDIA will continue to be a unique resource for understanding determinants, mechanisms, and outcomes of cardiovascular health and disease across the life course, leveraging ongoing pan-omics work from genomics to metabolomics that will define mechanistic pathways involved in cardiometabolic aging.
Keywords: cardiovascular disease; cardiovascular health; cardiovascular risk factors; race; social determinants of health.
Copyright © 2021 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures CARDIA is supported by contracts HHSN268201800003I, HHSN268201800004I, HHSN268201800005I, HHSN268201800006I, and HHSN268201800007I from the National Heart, Lung, and Blood Institute. The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute, the National Institutes of Health, or the U.S. Department of Health and Human Services. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Friedman GD, Cutter GR, Donahue RP, et al. CARDIA: study design, recruitment, and some characteristics of the examined subjects. J Clin Epidemiol 1988;41:1105–16. - PubMed
-
- Jacobs DR Jr., Hannan PJ, Wallace D, Liu K, Williams OD, Lewis CE. Interpreting age, period and cohort effects in plasma lipids and serum insulin using repeated measures regression analysis: the CARDIA Study. Stat Med 1999;18:655–79. - PubMed
-
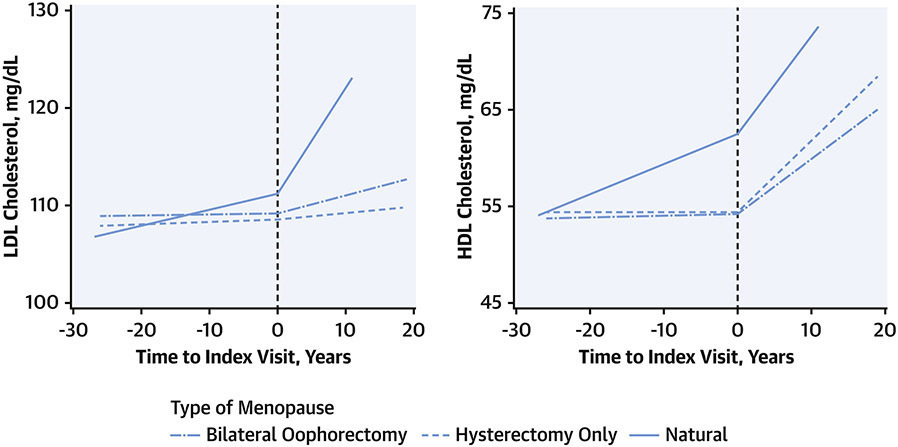
- Domanski MJ, Tian X, Wu CO, et al. Time Course of LDL Cholesterol Exposure and Cardiovascular Disease Event Risk. J Am Coll Cardiol 2020;76:1507–1516. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
