

A Phase I Trial of Regional Mesothelin-Targeted CAR T-cell Therapy in Patients with Malignant Pleural Disease, in Combination with the Anti-PD-1 Agent Pembrolizumab
- PMID: 34266984
- PMCID: PMC8563385
- DOI: 10.1158/2159-8290.CD-21-0407
A Phase I Trial of Regional Mesothelin-Targeted CAR T-cell Therapy in Patients with Malignant Pleural Disease, in Combination with the Anti-PD-1 Agent Pembrolizumab
Abstract
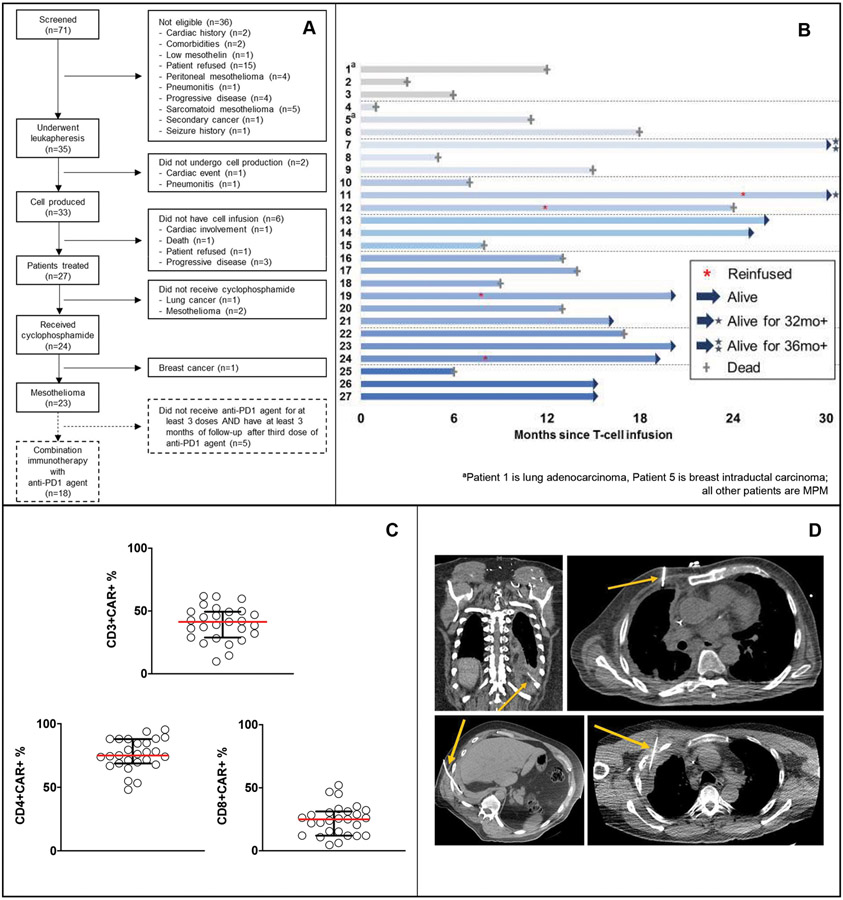
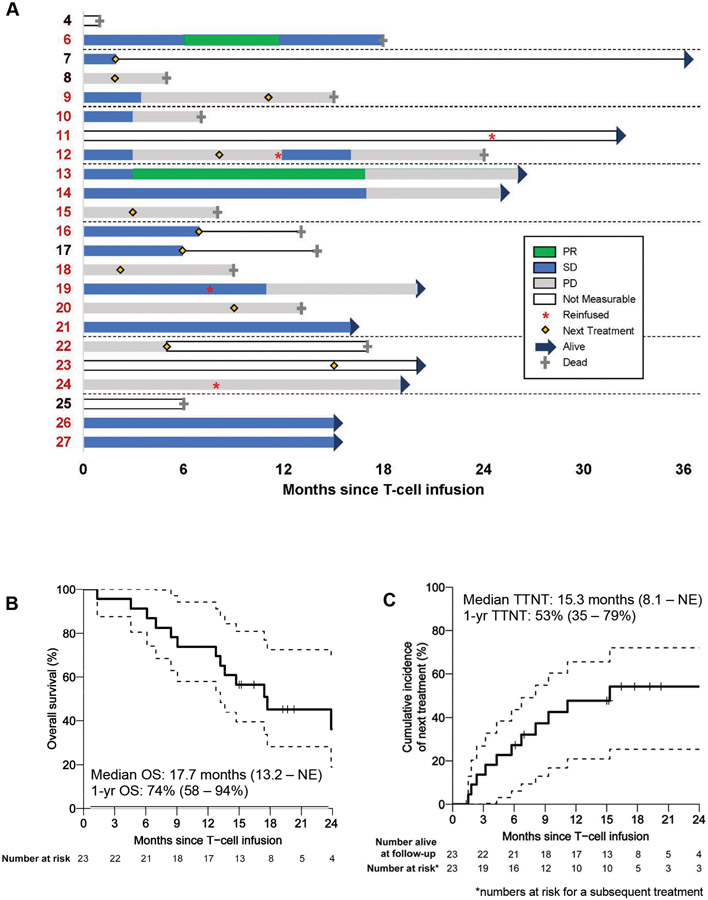
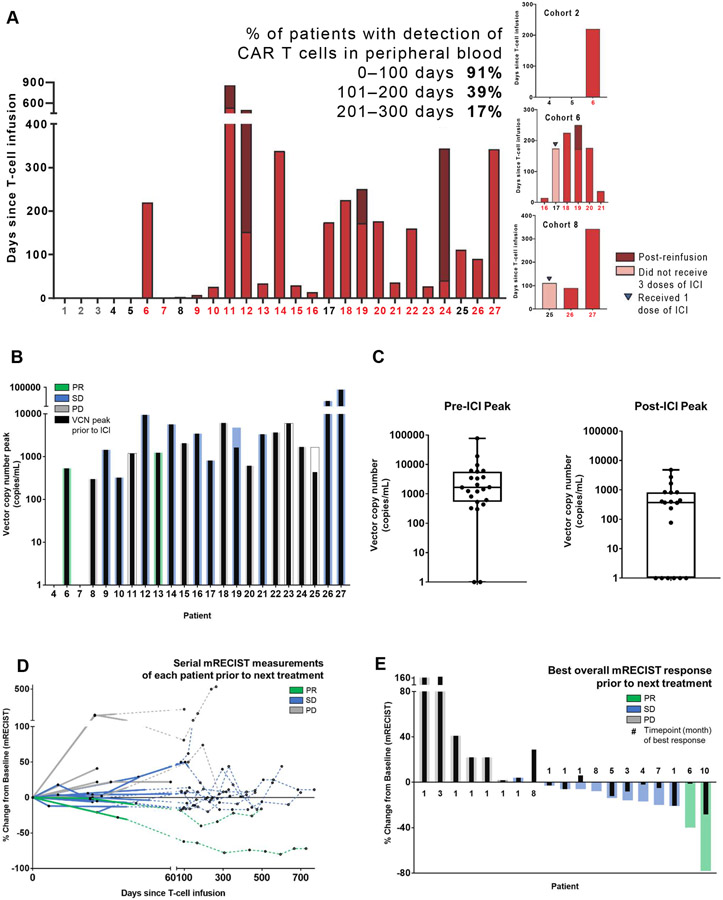
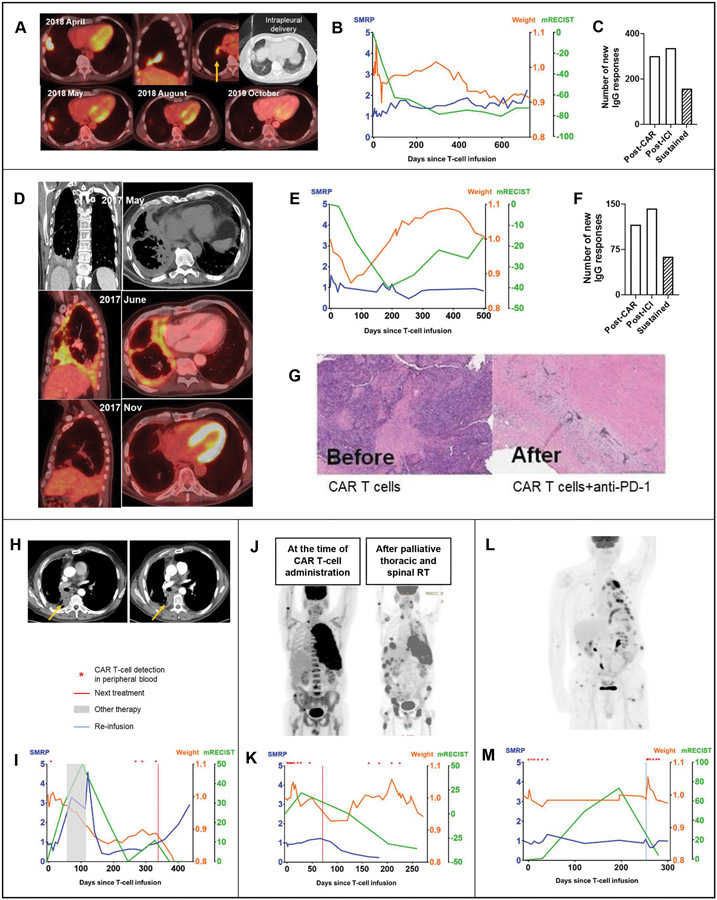
Malignant pleural diseases, comprising metastatic lung and breast cancers and malignant pleural mesothelioma (MPM), are aggressive solid tumors with poor therapeutic response. We developed and conducted a first-in-human, phase I study of regionally delivered, autologous, mesothelin-targeted chimeric antigen receptor (CAR) T-cell therapy. Intrapleural administration of 0.3M to 60M CAR T cells/kg in 27 patients (25 with MPM) was safe and well tolerated. CAR T cells were detected in peripheral blood for >100 days in 39% of patients. Following our demonstration that PD-1 blockade enhances CAR T-cell function in mice, 18 patients with MPM also received pembrolizumab safely. Among those patients, median overall survival from CAR T-cell infusion was 23.9 months (1-year overall survival, 83%). Stable disease was sustained for ≥6 months in 8 patients; 2 exhibited complete metabolic response on PET scan. Combination immunotherapy with CAR T cells and PD-1 blockade agents should be further evaluated in patients with solid tumors. SIGNIFICANCE: Regional delivery of mesothelin-targeted CAR T-cell therapy followed by pembrolizumab administration is feasible, safe, and demonstrates evidence of antitumor efficacy in patients with malignant pleural diseases. Our data support the investigation of combination immunotherapy with CAR T cells and PD-1 blockade agents in solid tumors.See related commentary by Aldea et al., p. 2674.This article is highlighted in the In This Issue feature, p. 2659.
©2021 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
CAR T cells show promise in mesothelioma.Nat Rev Clin Oncol. 2021 Sep;18(9):541. doi: 10.1038/s41571-021-00547-4. Nat Rev Clin Oncol. 2021. PMID: 34312528 No abstract available.
-
New Immunotherapy Combinations Enter the Battlefield of Malignant Mesothelioma.Cancer Discov. 2021 Nov;11(11):2674-2676. doi: 10.1158/2159-8290.CD-21-1046. Cancer Discov. 2021. PMID: 34725087
References
-
- Vogelzang NJ, Rusthoven JJ, Symanowski J, Denham C, Kaukel E, Ruffie P, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol 2003;21(14):2636–44. - PubMed
-
- Zalcman G, Mazieres J, Margery J, Greillier L, Audigier-Valette C, Moro-Sibilot D, et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): a randomised, controlled, open-label, phase 3 trial. Lancet 2016;387(10026):1405–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
