

Stable Gastric Pentadecapeptide BPC 157 and Wound Healing
- PMID: 34267654
- PMCID: PMC8275860
- DOI: 10.3389/fphar.2021.627533
Stable Gastric Pentadecapeptide BPC 157 and Wound Healing
Abstract
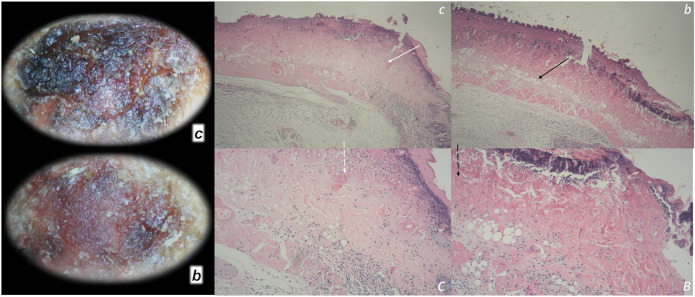
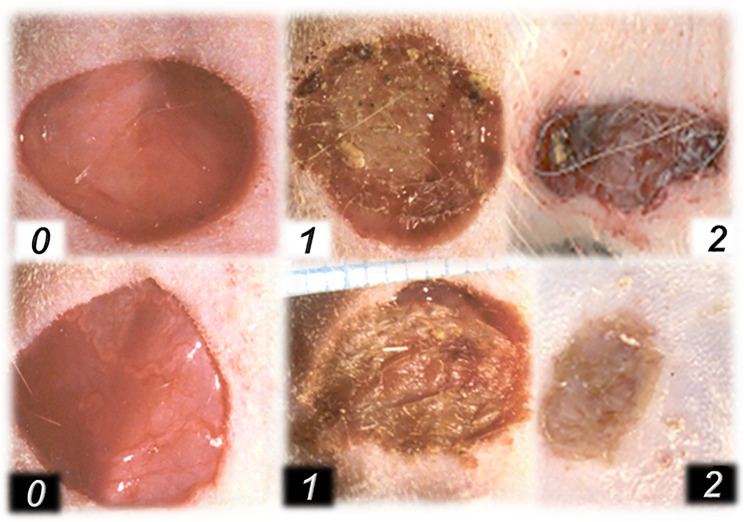
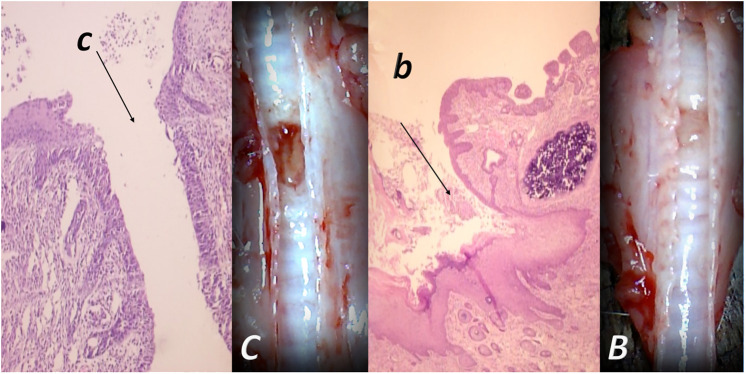
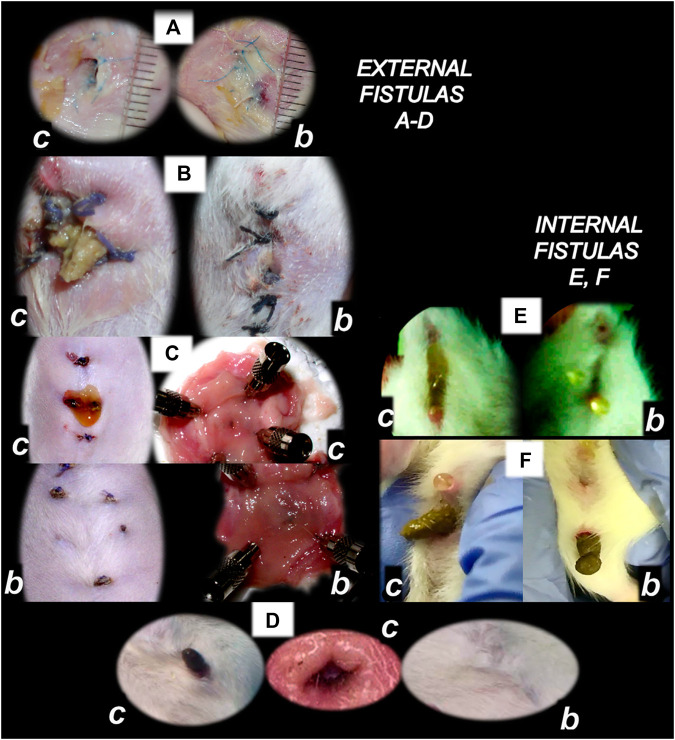
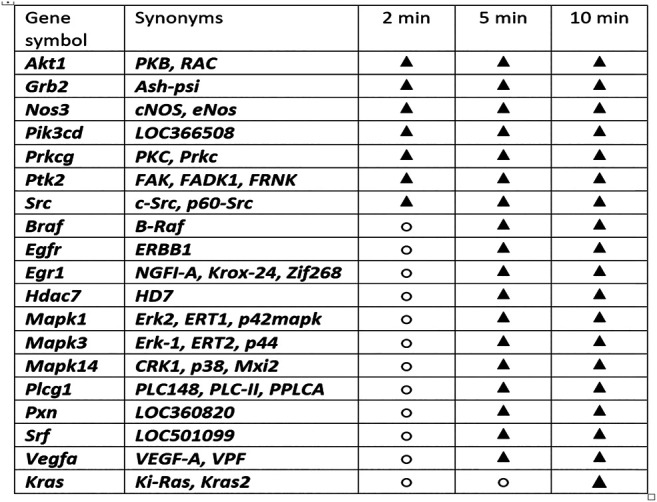
Significance: The antiulcer peptide, stable gastric pentadecapeptide BPC 157 (previously employed in ulcerative colitis and multiple sclerosis trials, no reported toxicity (LD1 not achieved)), is reviewed, focusing on the particular skin wound therapy, incisional/excisional wound, deep burns, diabetic ulcers, and alkali burns, which may be generalized to the other tissues healing. Recent Advances: BPC 157 has practical applicability (given alone, with the same dose range, and same equipotent routes of application, regardless the injury tested). Critical Issues: By simultaneously curing cutaneous and other tissue wounds (colocutaneous, gastrocutaneous, esophagocutaneous, duodenocutaneous, vesicovaginal, and rectovaginal) in rats, the potency of BPC 157 is evident. Healing of the wounds is accomplished by resolution of vessel constriction, the primary platelet plug, the fibrin mesh which acts to stabilize the platelet plug, and resolution of the clot. Thereby, BPC 157 is effective in wound healing much like it is effective in counteracting bleeding disorders, produced by amputation, and/or anticoagulants application. Likewise, BPC 157 may prevent and/or attenuate or eliminate, thus, counteract both arterial and venous thrombosis. Then, confronted with obstructed vessels, there is circumvention of the occlusion, which may be the particular action of BPC 157 in ischemia/reperfusion. Future Directions: BPC 157 rapidly increases various genes expression in rat excision skin wound. This would define the healing in the other tissues, that is, gastrointestinal tract, tendon, ligament, muscle, bone, nerve, spinal cord, cornea (maintained transparency), and blood vessels, seen with BPC 157 therapy.
Keywords: bleeding disorder; concept practical applicability; fistula; stable gastric pentadecapeptide BPC 157; wound healing.
Copyright © 2021 Seiwerth, Milavic, Vukojevic, Gojkovic, Krezic, Vuletic, Pavlov, Petrovic, Sikiric, Vranes, Prtoric, Zizek, Durasin, Dobric, Staresinic, Strbe, Knezevic, Sola, Kokot, Sever, Lovric, Skrtic, Blagaic and Sikiric.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Amic F., Drmic D., Bilic Z., Krezic I., Zizek H., Peklic M., et al. (2018). Bypassing major venous occlusion and duodenal lesions in rats, and therapy with the stable gastric pentadecapeptide BPC 157, L-NAME and L-arginine. World J. Gastroenterol. 24 (47), 5366–5378. 10.3748/wjg.v24.i47.5366 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources