

Limitations of a Commercial Assay as Diagnostic Test of Autoimmune Encephalitis
- PMID: 34267758
- PMCID: PMC8276168
- DOI: 10.3389/fimmu.2021.691536
Limitations of a Commercial Assay as Diagnostic Test of Autoimmune Encephalitis
Abstract
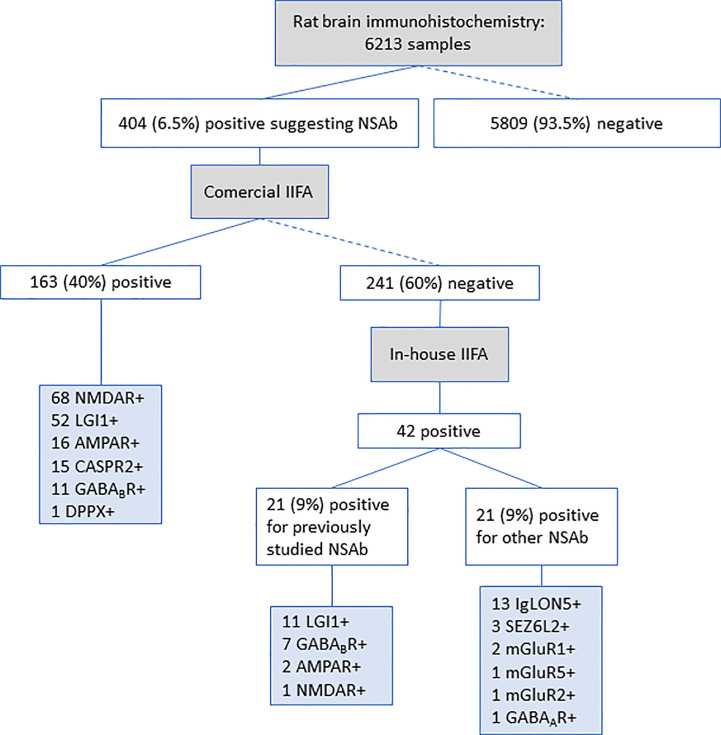
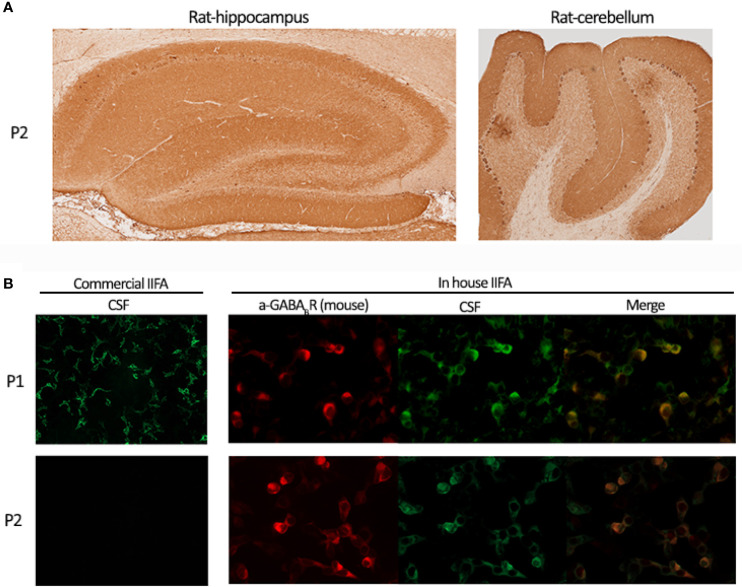
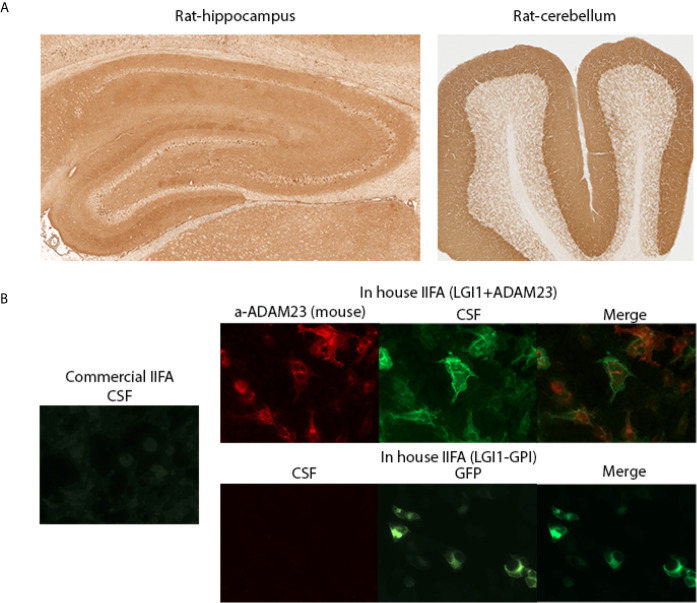
Detection of neuronal surface antibodies (NSAb) is important for the diagnosis of autoimmune encephalitis (AE). Although most clinical laboratories use a commercial diagnostic kit (Euroimmun, Lübeck, Germany) based on indirect immunofluorescence on transfected cells (IIFA), clinical experience suggests diagnostic limitations. Here, we assessed the performance of the commercial IIFA in serum and CSF samples of patients with suspected AE previously examined by rat brain immunohistochemistry (Cohort A). Of 6213 samples, 404 (6.5%) showed brain immunostaining suggestive of NSAb: 163 (40%) were positive by commercial IIFA and 241 (60%) were negative. When these 241 samples were re-assessed with in-house IIFA, 42 (18%) were positive: 21 (9%) had NSAb against antigens not included in the commercial IIFA and the other 21 (9%) had NSAb against antigens included in the commercial kit (false negative results). False negative results occurred more frequently with CSF (29% vs 10% in serum) and predominantly affected GABABR (39%), LGI1 (17%) and AMPAR (11%) antibodies. Results were reproduced in a separate cohort (B) of 54 AE patients with LGI1, GABABR or AMPAR antibodies in CSF which were missed in 30% by commercial IIFA. Patients with discordant GABABR antibody results (positive in-house but negative commercial IIFA) were less likely to develop full-blown clinical syndrome; no significant clinical differences were noted for the other antibodies. Overall, NSAb testing by commercial IIFA led to false negative results in a substantial number of patients, mainly those affected by anti-LG1, GABABR or AMPAR encephalitis. If these disorders are suspected and commercial IIFA is negative, more comprehensive antibody studies are recommended.
Keywords: autoimmune encephalitis (AE); brain immunohistochemistry; diagnostic test; immunofluorescent assay; neuronal antibodies.
Copyright © 2021 Ruiz-García, Muñoz-Sánchez, Naranjo, Guasp, Sabater, Saiz, Dalmau, Graus and Martinez-Hernandez.
Conflict of interest statement
JD receives royalties from Athena Diagnostics for the use of Ma2 as an autoantibody test and from Euroimmun for the use of NMDA, GABAB receptor, GABAA receptor, DPPX and IgLON5 as autoantibody tests. FG holds a patent for the use of IgLON5 as an autoantibody test. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor declared a past co-authorship with the authors FG and JD.
Figures
References
-
- Dalmau J, Graus F. Antibody-Mediated Encephalitis. (2018) (Accessed 2019 Aug 15). - PubMed