

Glioblastoma Shortly after a Normal Conventional Brain Magnetic Resonance Imaging: A Report of Two Cases and Review of the Literature
- PMID: 34268181
- PMCID: PMC8244693
- DOI: 10.4103/ajns.AJNS_553_20
Glioblastoma Shortly after a Normal Conventional Brain Magnetic Resonance Imaging: A Report of Two Cases and Review of the Literature
Abstract
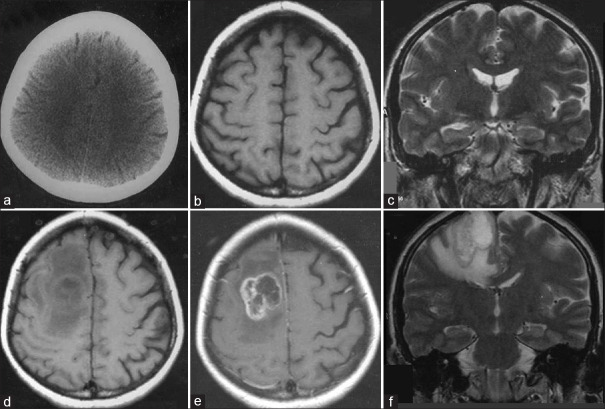
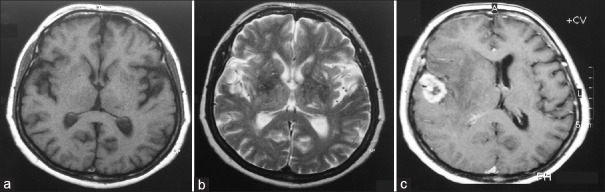
Glioblastoma (GB) is the most common malignant tumor of the brain. Most of these tumors are primary or de novo GBs that manifest rapidly with initial presentations such as headache, new-onset epileptic seizure, focal neurological deficits, and altered mental status. The typical radiological features of GB include strong contrast enhancement, central necrosis, and edema with mass effect. Herein, we describe two cases of primary GB - two women aged 60 and 51 years who were diagnosed with GB 3.5 and 4 months, respectively, after their initial admission. These patients presented with right-sided headaches, and their neurological examination was within the normal limits. Their initial radiological investigations revealed no suspicious lesions, either on T1-weighted or T2-weighted magnetic resonance (MR) images. The 60-year-old patient was readmitted with persistent headache, and her T1-weighted MR images revealed a well-demarcated mass lesion in the right temporal lobe with strong contrast enhancement. Moreover, the T2-weighted MR images revealed closed sulci and swollen midline structures because of edema. The 51-year-old patient was readmitted with persistent headache, and her MR image revealed a mass lesion with heterogeneous contrast enhancement and necrosis on T1-weighted images and hyperintense areas with severe edema on T2-weighted images. The patients underwent craniotomy and gross total tumor resection. Notably, in both cases, the lesions were pathologically diagnosed as GB. Therefore, it should be borne in mind that only persistent headache could be a sentinel sign of GB before it becomes radiologically visible, thereby emphasizing the need for follow-up imaging studies at short intervals.
Keywords: Cerebral imaging; diagnosis; glioblastoma; headache; magnetic resonance imaging; occult brain tumor.
Copyright: © 2021 Asian Journal of Neurosurgery.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Transient MR signal changes in patients with generalized tonicoclonic seizure or status epilepticus: periictal diffusion-weighted imaging.AJNR Am J Neuroradiol. 2001 Jun-Jul;22(6):1149-60. AJNR Am J Neuroradiol. 2001. PMID: 11415912 Free PMC article.
-
Early stage glioblastoma: retrospective multicentric analysis of clinical and radiological features.Radiol Med. 2021 Nov;126(11):1468-1476. doi: 10.1007/s11547-021-01401-4. Epub 2021 Aug 2. Radiol Med. 2021. PMID: 34338949
-
[Diffusion weighted MR: principles and clinical use in selected brain diseases].Radiol Med. 2000 Dec;100(6):470-9. Radiol Med. 2000. PMID: 11307509 Italian.
-
Magnetic Resonance Imaging Features in Solitary Cerebral Langerhans Cell Histiocytosis: Case Report and Review of Literature.World Neurosurg. 2018 Aug;116:333-336. doi: 10.1016/j.wneu.2018.06.060. Epub 2018 Jun 19. World Neurosurg. 2018. PMID: 29929024 Review.
-
[Glioblastoma multiforme developing separately from the initial lesion 9 years after successful treatment for gliomatosis cerebri: a case report].No Shinkei Geka. 2008 Aug;36(8):709-15. No Shinkei Geka. 2008. PMID: 18700534 Review. Japanese.
Cited by
-
Within five weeks: Rapidly grown glioblastoma discovered on repeat MRI after pathologic EEG.Clin Neurophysiol Pract. 2025 Feb 22;10:52-55. doi: 10.1016/j.cnp.2025.02.002. eCollection 2025. Clin Neurophysiol Pract. 2025. PMID: 40092495 Free PMC article.
References
-
- Weller M, van den Bent M, Tonn JC, Stupp R, Preusser M, Cohen-Jonathan-Moyal E, et al. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017;18:e315–29. - PubMed
-
- Chittiboina P, Connor DE, Caldito G, Quillin JW, Wilson JD, Nanda A. Occult tumors presenting with negative imaging: Analysis of the literature: A review. J Neurosurg. 2021;116:1195–203. - PubMed
-
- Schröter N, Lützen N, Doostkam S, Berger B. Int J Neurosci. 2020. Glioblastoma evolving within 10 days following unremarkable computer tomography of the brain: A case report; pp. 1–4. doi: 10.1080/00207454.2020.1753730. - PubMed