

Gastric epithelial neoplasm of fundic-gland mucosa lineage: proposal for a new classification in association with gastric adenocarcinoma of fundic-gland type
- PMID: 34268625
- PMCID: PMC8370942
- DOI: 10.1007/s00535-021-01813-z
Gastric epithelial neoplasm of fundic-gland mucosa lineage: proposal for a new classification in association with gastric adenocarcinoma of fundic-gland type
Abstract
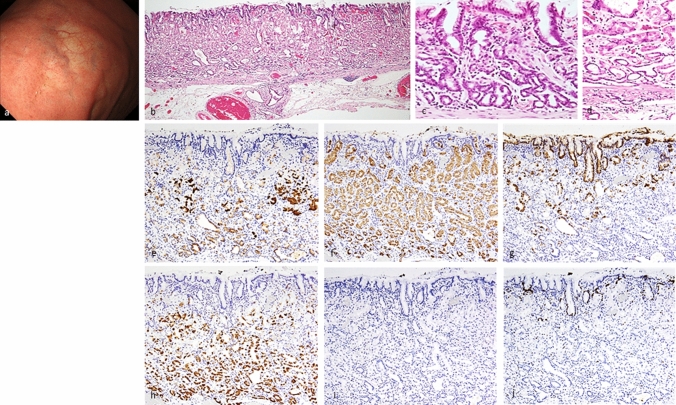
Background: Gastric adenocarcinoma of fundic-gland type (GA-FG) is a rare variant of gastric neoplasia. However, the etiology, classification, and clinicopathological features of gastric epithelial neoplasm of fundic-gland mucosa lineage (GEN-FGML; generic term of GA-FG related neoplasm) are not fully elucidated. We performed a large, multicenter, retrospective study to establish a new classification and clarify the clinicopathological features of GEN-FGML.
Methods: One hundred GEN-FGML lesions in 94 patients were collected from 35 institutions between 2008 and 2019. We designed a new histopathological classification of GEN-FGML using immunohistochemical analysis and analyzed via clinicopathological, immunohistochemical, and genetic evaluation.
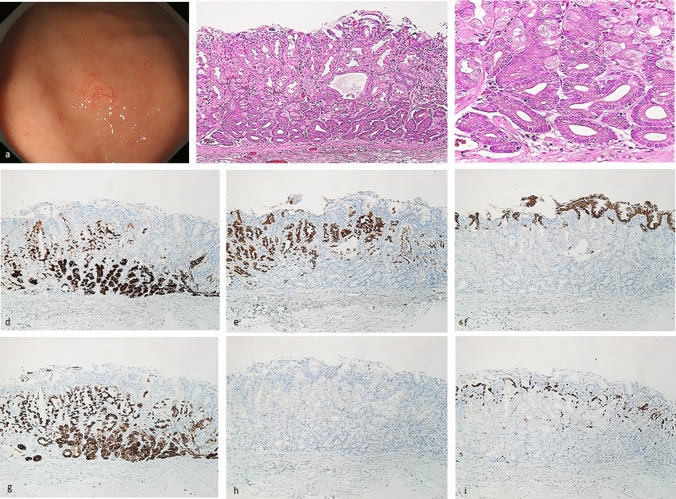
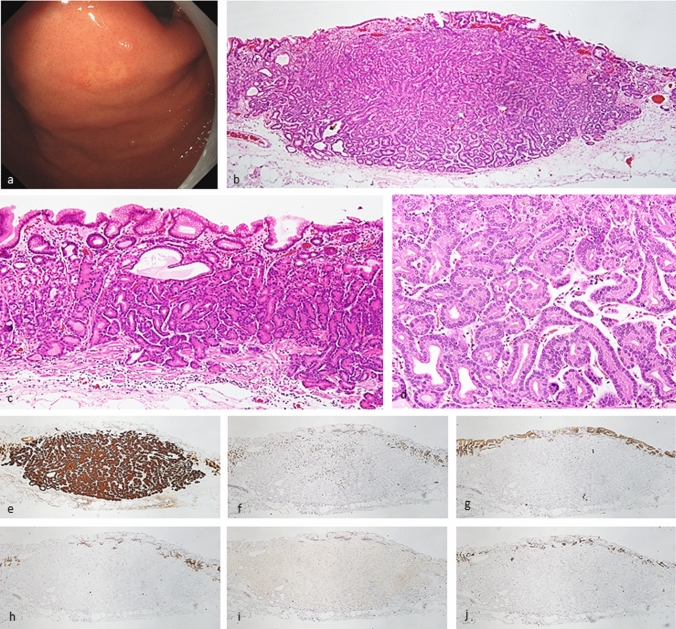
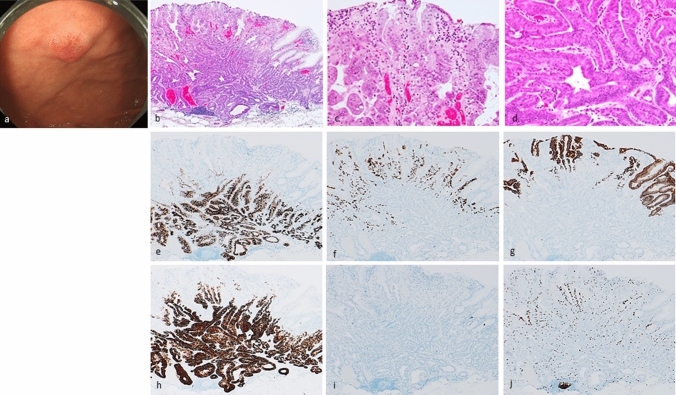
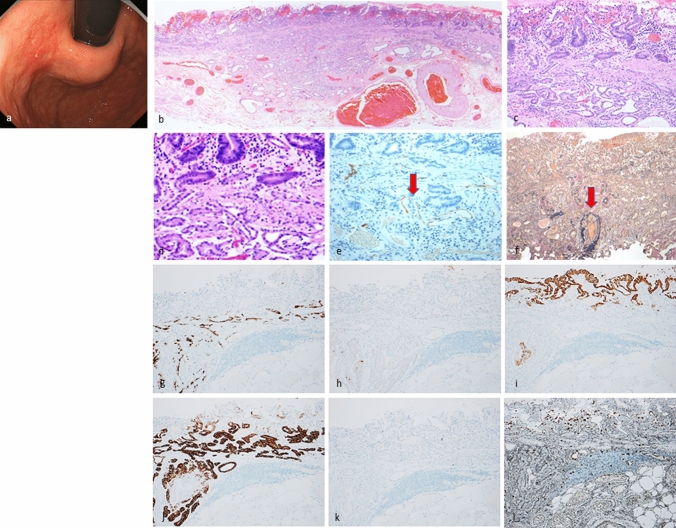
Results: GEN-FGML was classified into 3 major types; oxyntic gland adenoma (OGA), GA-FG, and gastric adenocarcinoma of fundic-gland mucosa type (GA-FGM). In addition, GA-FGM was classified into 3 subtypes; Type 1 (organized with exposure type), Type 2 (disorganized with exposure type), and Type 3 (disorganized with non-exposure type). OGA and GA-FG demonstrated low-grade epithelial neoplasm, and GA-FGM should be categorized as an aggressive variant of GEN-FGML that demonstrated high-grade epithelial neoplasm (Type 2 > 1, 3). The frequent presence of GNAS mutation was a characteristic genetic feature of GEN-FGML (7/34, 20.6%; OGA 1/3, 33.3%; GA-FG 3/24, 12.5%; GA-FGM 3/7, 42.9%) in mutation analysis using next-generation sequencing.
Conclusions: We have established a new histopathological classification of GEN-FGML and propose a new lineage of gastric epithelial neoplasm that harbors recurrent GNAS mutation. This classification will be useful to estimate the malignant potential of GEN-FGML and establish an appropriate standard therapeutic approach.
Keywords: Gastric adenocarcinoma of fundic-gland mucosa type; Gastric adenocarcinoma of fundic-gland type; Gastric epithelial neoplasm of fundic-gland mucosa lineage; Oxyntic gland adenoma.
© 2021. The Author(s).
Conflict of interest statement
All authors have no financial relationships relevant to this publication.
Figures
References
-
- Ueyama H, Yao T, Matsumoto K, et al. Establishment of endoscopic diagnosis for gastric adenocarcinoma of fundic gland type (chief cell predominant type) using magnifying endoscopy with narrow-band imaging. Stomach Intest. 2015;50:1533–1547.
-
- Ueyama H, Matsumoto K, Nagahara A, et al. Core tips for the endoscopic diagnosis of gastric adenocarcinoma of fundic gland type (chief cell predominant type) Gastrointest Endosc. 2016;58:1169–1177.
-
- Ueyama H, Yao T, Matsumoto K, et al. Gastric adenocarcinoma of fundic gland type. Stomach Intest. 2018;53:753–767.
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
