

COVID-19 infection, progression, and vaccination: Focus on obesity and related metabolic disturbances
- PMID: 34269511
- PMCID: PMC8420274
- DOI: 10.1111/obr.13313
COVID-19 infection, progression, and vaccination: Focus on obesity and related metabolic disturbances
Abstract
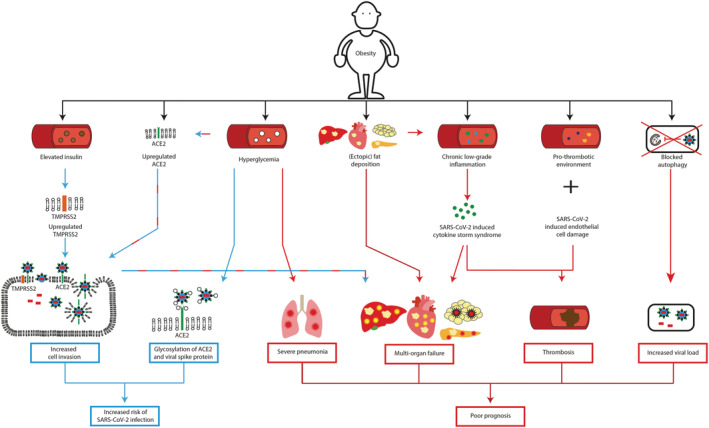
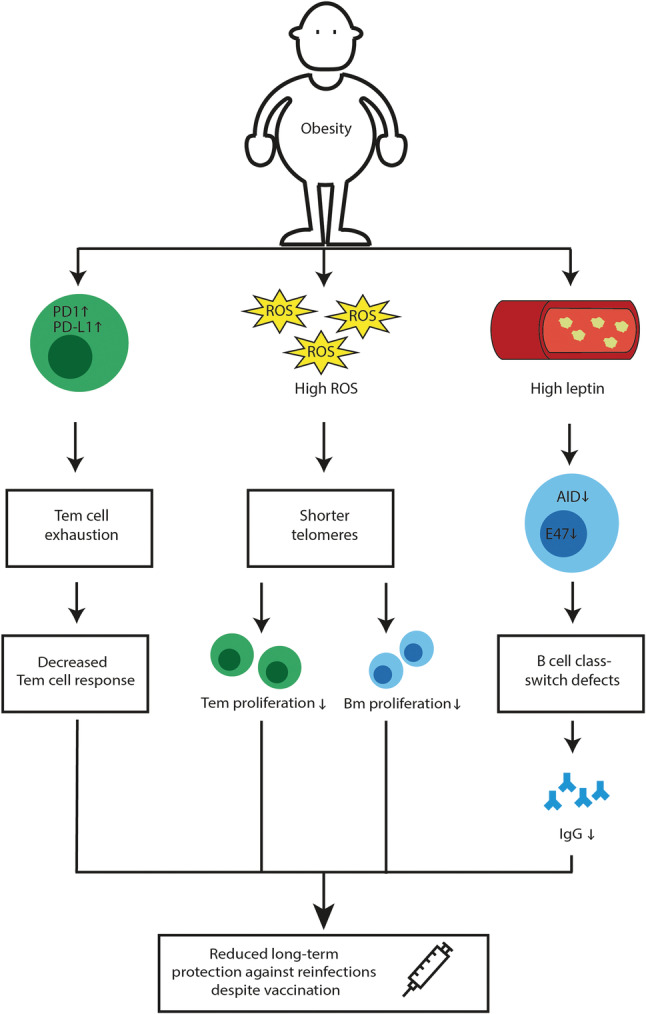
Coronaviruses are constantly circulating in humans, causing common colds and mild respiratory infections. In contrast, infection with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for coronavirus disease-2019 (COVID-19), can cause additional severe complications, particularly in patients with obesity and associated metabolic disturbances. Obesity is a principal causative factor in the development of the metabolic syndrome; a series of physiological, biochemical, clinical, and metabolic factors that increase the risk of obesity-associated diseases. "Metabolically unhealthy" obesity is, in addition to metabolic disturbances, also associated with immunological disturbances. As such, patients with obesity are more prone to develop serious complications from infections, including those from SARS-CoV-2. In this review, we first describe how obesity and related metabolic disturbances increase the risk of SARS-CoV-2 infection. Then, mechanisms contributing to COVID-19 complications and poor prognosis in these patients are discussed. Finally, we discuss how obesity potentially reduces long-term COVID-19 vaccination efficacy. Despite encouraging COVID-19 vaccination results in patients with obesity and related metabolic disturbances in the short-term, it is becoming increasingly evident that long-term COVID-19 vaccination efficacy should be closely monitored in this vulnerable group.
Keywords: COVID-19; metabolic syndrome; obesity; severe acute respiratory syndrome coronavirus 2.
© 2021 The Authors. Obesity Reviews published by John Wiley & Sons Ltd on behalf of World Obesity Federation.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent‐licensing arrangements), or non‐financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
-
- WHO . https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019?gclid=EA.... Accessed March 3, 2021.
-
- Hodinka RL. Respiratory RNA viruses. Microbiol Spectr. 2016;4(4):1‐33. - PubMed
-
- Jean A, Quach C, Yung A, Semret M. Severity and outcome associated with human coronavirus OC43 infections among children. Pediatr Infect Dis J. 2013;32(4):325‐329. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
