

Mortality from gastrointestinal congenital anomalies at 264 hospitals in 74 low-income, middle-income, and high-income countries: a multicentre, international, prospective cohort study
- PMID: 34270932
- PMCID: PMC8314066
- DOI: 10.1016/S0140-6736(21)00767-4
Mortality from gastrointestinal congenital anomalies at 264 hospitals in 74 low-income, middle-income, and high-income countries: a multicentre, international, prospective cohort study
Abstract
Background: Congenital anomalies are the fifth leading cause of mortality in children younger than 5 years globally. Many gastrointestinal congenital anomalies are fatal without timely access to neonatal surgical care, but few studies have been done on these conditions in low-income and middle-income countries (LMICs). We compared outcomes of the seven most common gastrointestinal congenital anomalies in low-income, middle-income, and high-income countries globally, and identified factors associated with mortality.
Methods: We did a multicentre, international prospective cohort study of patients younger than 16 years, presenting to hospital for the first time with oesophageal atresia, congenital diaphragmatic hernia, intestinal atresia, gastroschisis, exomphalos, anorectal malformation, and Hirschsprung's disease. Recruitment was of consecutive patients for a minimum of 1 month between October, 2018, and April, 2019. We collected data on patient demographics, clinical status, interventions, and outcomes using the REDCap platform. Patients were followed up for 30 days after primary intervention, or 30 days after admission if they did not receive an intervention. The primary outcome was all-cause, in-hospital mortality for all conditions combined and each condition individually, stratified by country income status. We did a complete case analysis.
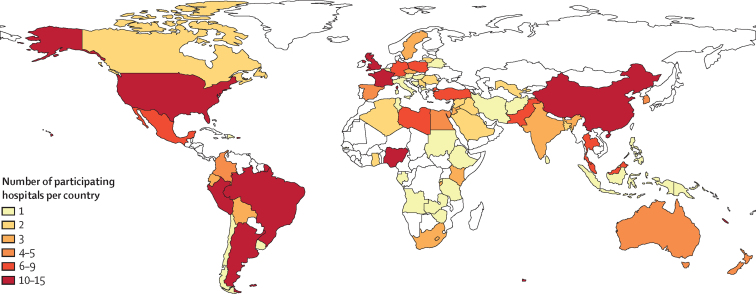
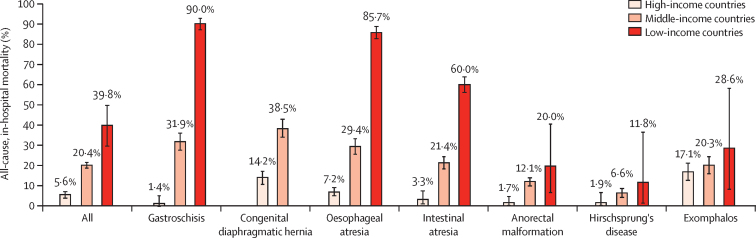
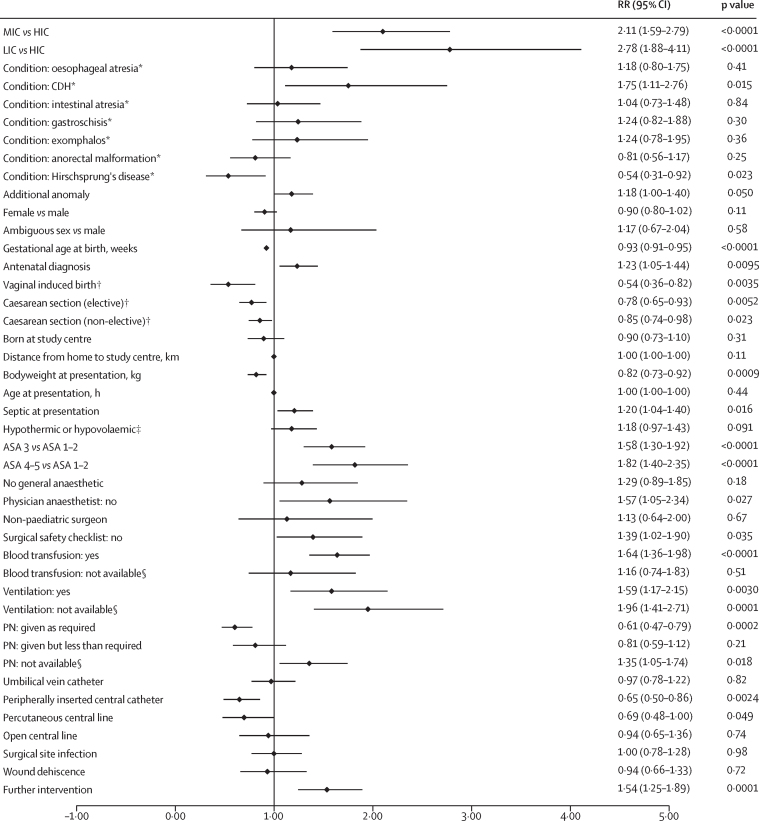
Findings: We included 3849 patients with 3975 study conditions (560 with oesophageal atresia, 448 with congenital diaphragmatic hernia, 681 with intestinal atresia, 453 with gastroschisis, 325 with exomphalos, 991 with anorectal malformation, and 517 with Hirschsprung's disease) from 264 hospitals (89 in high-income countries, 166 in middle-income countries, and nine in low-income countries) in 74 countries. Of the 3849 patients, 2231 (58·0%) were male. Median gestational age at birth was 38 weeks (IQR 36-39) and median bodyweight at presentation was 2·8 kg (2·3-3·3). Mortality among all patients was 37 (39·8%) of 93 in low-income countries, 583 (20·4%) of 2860 in middle-income countries, and 50 (5·6%) of 896 in high-income countries (p<0·0001 between all country income groups). Gastroschisis had the greatest difference in mortality between country income strata (nine [90·0%] of ten in low-income countries, 97 [31·9%] of 304 in middle-income countries, and two [1·4%] of 139 in high-income countries; p≤0·0001 between all country income groups). Factors significantly associated with higher mortality for all patients combined included country income status (low-income vs high-income countries, risk ratio 2·78 [95% CI 1·88-4·11], p<0·0001; middle-income vs high-income countries, 2·11 [1·59-2·79], p<0·0001), sepsis at presentation (1·20 [1·04-1·40], p=0·016), higher American Society of Anesthesiologists (ASA) score at primary intervention (ASA 4-5 vs ASA 1-2, 1·82 [1·40-2·35], p<0·0001; ASA 3 vs ASA 1-2, 1·58, [1·30-1·92], p<0·0001]), surgical safety checklist not used (1·39 [1·02-1·90], p=0·035), and ventilation or parenteral nutrition unavailable when needed (ventilation 1·96, [1·41-2·71], p=0·0001; parenteral nutrition 1·35, [1·05-1·74], p=0·018). Administration of parenteral nutrition (0·61, [0·47-0·79], p=0·0002) and use of a peripherally inserted central catheter (0·65 [0·50-0·86], p=0·0024) or percutaneous central line (0·69 [0·48-1·00], p=0·049) were associated with lower mortality.
Interpretation: Unacceptable differences in mortality exist for gastrointestinal congenital anomalies between low-income, middle-income, and high-income countries. Improving access to quality neonatal surgical care in LMICs will be vital to achieve Sustainable Development Goal 3.2 of ending preventable deaths in neonates and children younger than 5 years by 2030.
Funding: Wellcome Trust.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests NS is the director of the London Safety and Training Solutions, which offers training in patient safety, implementation solutions, and human factors to health-care organisations. All other authors declare no competing interests.
Figures

Comment in
-
Paediatric surgery for congenital anomalies: the next frontier for global health.Lancet. 2021 Jul 24;398(10297):280-281. doi: 10.1016/S0140-6736(21)01547-6. Epub 2021 Jul 13. Lancet. 2021. PMID: 34270931 No abstract available.
References
-
- The Lancet Every Newborn Study Group Lancet Every Newborn Series. 2014. https://www.thelancet.com/series/everynewborn
-
- WHO Children: improving survival and well-being. Sept 8, 2020. https://www.who.int/en/news-room/fact-sheets/detail/children-reducing-mo...
-
- Wright NJ, Anderson JE, Ozgediz D, Farmer DL, Banu T. Addressing paediatric surgical care on World Birth Defects Day. Lancet. 2018;391 - PubMed
-
- WHO Congenital anomalies. 2016. https://www.who.int/en/news-room/fact-sheets/detail/congenital-anomalies
-
- Institute of Health Metrics and Evaluation GBD results tool. Congenital anomaly deaths, globally, both sexes, under 5-years, 2015. 2019. http://ghdx.healthdata.org/gbd-results-tool
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
