

Improving statin treatment strategies to reduce LDL-cholesterol: factors associated with targets' attainment in subjects with and without type 2 diabetes
- PMID: 34271920
- PMCID: PMC8283985
- DOI: 10.1186/s12933-021-01338-y
Improving statin treatment strategies to reduce LDL-cholesterol: factors associated with targets' attainment in subjects with and without type 2 diabetes
Abstract
Background: This cross-sectional study aimed to identify actionable factors to improve LDL-cholesterol target achievement and overcome underuse of lipid-lowering treatments in high- or very-high-cardiovascular risk patients.
Methods: We evaluated healthcare records of 934,332 subjects from North-Italy, including subjects with available lipid profile and being on statin treatments up to December 2018. A 6-month-period defined adherence with proportion-of-days-covered ≥ 80%. Treatment was classified as high-intensity-statin (HIS) + ezetimibe, HIS-alone, non-HIS (NHIS) + ezetimibe or NHIS alone.
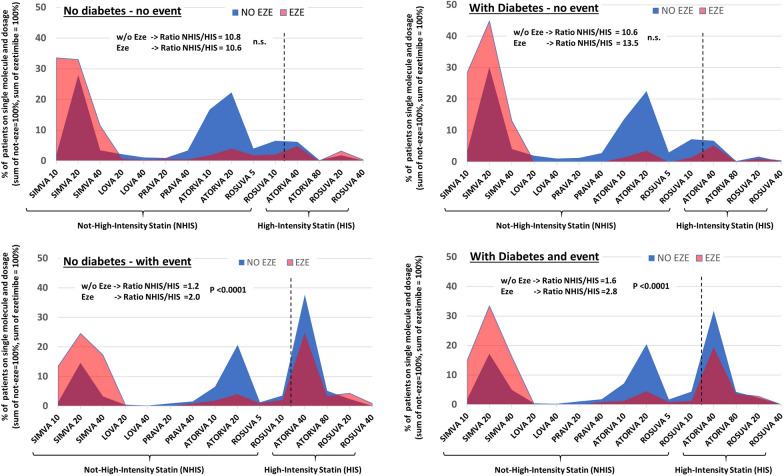
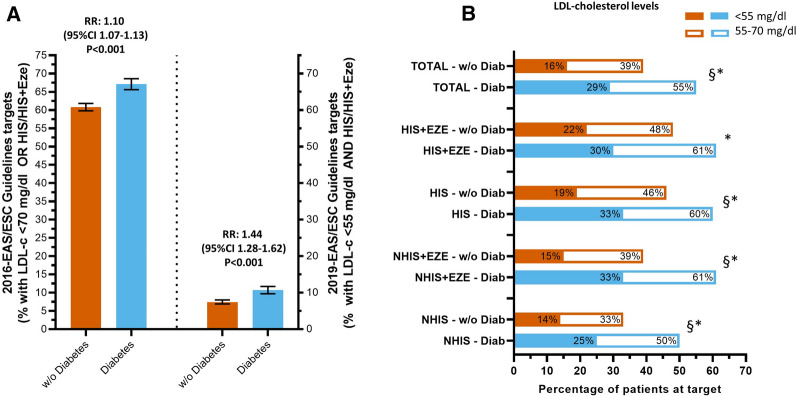
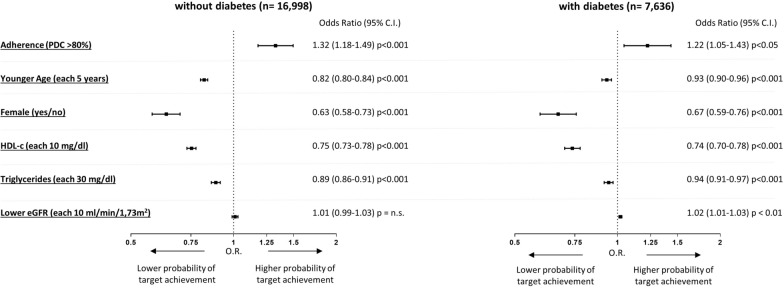
Results: We included 27,374 subjects without and 10,459 with diabetes. Among these, 30% and 36% were on secondary prevention, respectively. Adherence was high (78-100%) and increased with treatment intensity and in secondary prevention. Treatment intensity increased in secondary prevention, but only 42% were on HIS. 2019-guidelines LDL-cholesterol targets were achieved in few patients and more often among those with diabetes (7.4% vs. 10.7%, p < 0.001). Patients in secondary prevention had mean LDL-cholesterol levels aligned slightly above 70 mg/dl (range between 68 and 73 mg/dl and between 73 and 85 mg/dl in patients with and without diabetes, respectively). Moreover, the differences in mean LDL-cholesterol levels observed across patients using treatments with well-stablished different LDL-lowering effect were null or much smaller than expected (HIS vs. NHIS from - 3 to - 11%, p < 0.001, HIS + ezetimibe vs. HIS-from - 4 to + 5% n.s.). These findings, given the observational design of the study, might suggest that a "treat to absolute LDL-cholesterol levels" approach (e.g., targeting LDLc of 70 mg/dl) was mainly used by physicians rather than an approach to also achieve the recommended 50% reduction in LDL-cholesterol levels. Our analyses suggested that female sex, younger age, higher HDL-c, and elevated triglycerides are those factors delaying prescription of statin treatments, both in patients with and without diabetes and in those on secondary prevention.
Conclusions: Among patients on statin treatment and high adherence, only a small proportion of patients achieved LDL-cholesterol targets. Late initiation of high-intensity treatments, particularly among those with misperceived low-risk (e.g., female subjects or those with high HDL-cholesterol), appears as pivotal factors needing to be modified to improve CVD prevention.
Keywords: Cardiovascular prevention; Ezetimibe; Gender; HDL; PCSK9; Statins.
© 2021. The Author(s).
Conflict of interest statement
MLM received Grant support, lecture or consultant fees from Lilly, Merck Sharp & Dome, Mylan, Servier, Amryt and SLAPharma. AA received research grants, lecture or advisory board fees from Merck Sharp & Dome, AstraZeneca, Novartis, Boeringher-Ingelheim, Sanofi, Mediolanum, Janssen, Novo Nordisk, Lilly, Servier, Neopharmed Gentili, and Takeda.
Figures
References
-
- Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–72. doi: 10.1093/eurheartj/ehx144. - DOI - PMC - PubMed
-
- Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364(9435):685–96. doi: 10.1016/S0140-6736(04)16895-5. - DOI - PubMed
-
- Collins R, Armitage J, Parish S, Sleigh P, Peto R, Heart Protection Study Collaborative G MRC/BHF heart protection study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361(9374):2005–16. doi: 10.1016/S0140-6736(03)13636-7. - DOI - PubMed
-
- Briel M, Nordmann AJ, Bucher HC. Statin therapy for prevention and treatment of acute and chronic cardiovascular disease: update on recent trials and metaanalyses. Curr Opin Lipidol. 2005;16(6):601–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
