

Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease
- PMID: 34271948
- PMCID: PMC8285851
- DOI: 10.1186/s12933-021-01343-1
Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease
Abstract
Background: Multiple modifiable risk factors for late complications in patients with diabetic kidney disease (DKD), including hyperglycemia, hypertension and dyslipidemia, increase the risk of a poor outcome. DKD is associated with a very high cardiovascular risk, which requires simultaneous treatment of these risk factors by implementing an intensified multifactorial treatment approach. However, the efficacy of a multifactorial intervention on major fatal/non-fatal cardiovascular events (MACEs) in DKD patients has been poorly investigated.
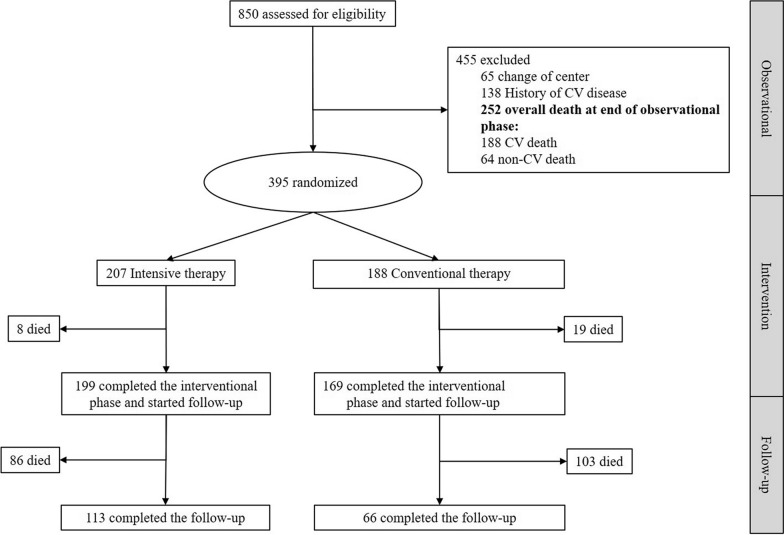
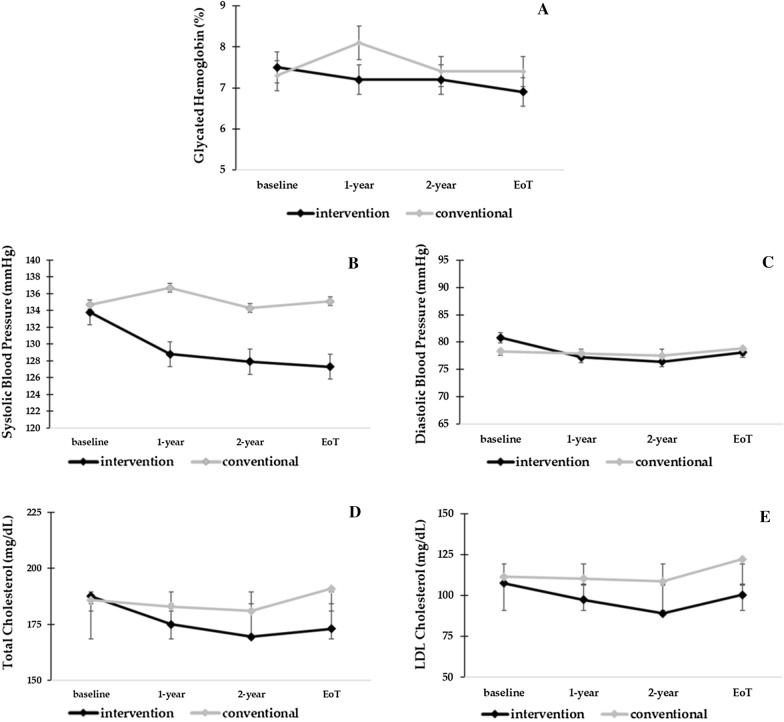
Methods: Nephropathy in Diabetes type 2 (NID-2) study is a multicentre, cluster-randomized, open-label clinical trial enrolling 395 DKD patients with albuminuria, diabetic retinopathy (DR) and negative history of CV events in 14 Italian diabetology clinics. Centres were randomly assigned to either Standard-of-Care (SoC) (n = 188) or multifactorial intensive therapy (MT, n = 207) of main cardiovascular risk factors (blood pressure < 130/80 mmHg, glycated haemoglobin < 7%, LDL, HDL and total cholesterol < 100 mg/dL, > 40/50 mg/dL for men/women and < 175 mg/dL, respectively). Primary endpoint was MACEs occurrence by end of follow-up phase. Secondary endpoints included single components of primary endpoint and all-cause death.
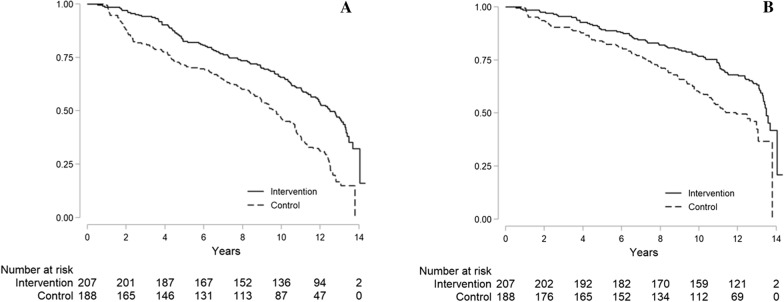
Results: At the end of intervention period (median 3.84 and 3.40 years in MT and SoC group, respectively), targets achievement was significantly higher in MT. During 13.0 years (IQR 12.4-13.3) of follow-up, 262 MACEs were recorded (116 in MT vs. 146 in SoC). The adjusted Cox shared-frailty model demonstrated 53% lower risk of MACEs in MT arm (adjusted HR 0.47, 95%CI 0.30-0.74, P = 0.001). Similarly, all-cause death risk was 47% lower (adjusted HR 0.53, 95%CI 0.29-0.93, P = 0.027).
Conclusion: MT induces a remarkable benefit on the risk of MACEs and mortality in high-risk DKD patients. Clinical Trial Registration ClinicalTrials.gov number, NCT00535925. https://clinicaltrials.gov/ct2/show/NCT00535925.
Keywords: CV risk factors; Diabetic nephropathy; Intensified treatment; MACE; Multifactorial intervention; Very high CV risk.
© 2021. The Author(s).
Conflict of interest statement
Luca De Nicola has received fees for scientific consultation and/or lectures by Astellas, AstraZeneca, Mundibiopharma and Vifor Pharma. Roberto Minutolo has been member of Advisory Boards for Astellas, and invited speaker at meetings supported by Amgen, Vifor Pharma. Ferdinando Carlo Sasso has been member of Advisory Boards for Boehringer and for Ely-Lilly and has received fees for scientific consultation and/or lectures by Jansen, Roche Diagnostics, Novo Nordisk, Sanofi, MSD, Astrazeneca. Pia Clara Pafundi, Vittorio Simeon, Paolo Chiodini, Raffaele Galiero, Luca Rinaldi, Riccardo Nevola, Teresa Salvatore, Raffaele Marfella, Celestino Sardu, and Luigi Elio Adinolfi have no conflict of interest to disclose.
Figures
References
-
- Fox CS, Matsushita K, Woodward M, et al. Chronic Kidney Disease Prognosis Consortium Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet. 2012;380(9854):1662–73. doi: 10.1016/S0140-6736(12)61350-6. - DOI - PMC - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154–69. doi: 10.1161/01.CIR.0000095676.90936.80. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
