

Personalized mechanical ventilation in acute respiratory distress syndrome
- PMID: 34271958
- PMCID: PMC8284184
- DOI: 10.1186/s13054-021-03686-3
Personalized mechanical ventilation in acute respiratory distress syndrome
Abstract
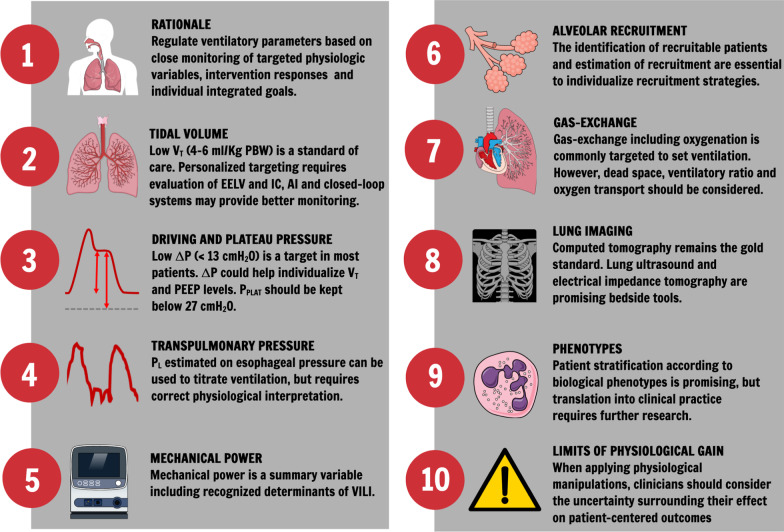
A personalized mechanical ventilation approach for patients with adult respiratory distress syndrome (ARDS) based on lung physiology and morphology, ARDS etiology, lung imaging, and biological phenotypes may improve ventilation practice and outcome. However, additional research is warranted before personalized mechanical ventilation strategies can be applied at the bedside. Ventilatory parameters should be titrated based on close monitoring of targeted physiologic variables and individualized goals. Although low tidal volume (VT) is a standard of care, further individualization of VT may necessitate the evaluation of lung volume reserve (e.g., inspiratory capacity). Low driving pressures provide a target for clinicians to adjust VT and possibly to optimize positive end-expiratory pressure (PEEP), while maintaining plateau pressures below safety thresholds. Esophageal pressure monitoring allows estimation of transpulmonary pressure, but its use requires technical skill and correct physiologic interpretation for clinical application at the bedside. Mechanical power considers ventilatory parameters as a whole in the optimization of ventilation setting, but further studies are necessary to assess its clinical relevance. The identification of recruitability in patients with ARDS is essential to titrate and individualize PEEP. To define gas-exchange targets for individual patients, clinicians should consider issues related to oxygen transport and dead space. In this review, we discuss the rationale for personalized approaches to mechanical ventilation for patients with ARDS, the role of lung imaging, phenotype identification, physiologically based individualized approaches to ventilation, and a future research agenda.
Keywords: Biomarkers; Chest computed tomography scan; Driving pressure; Phenotype; Tidal volume; Transpulmonary pressure.
© 2021. The Author(s).
Conflict of interest statement
JL discloses consultancy fees for Baxter and GlaxoSmithKline. JLT is member of the medical advisory board of Getinge. KB holds a Physician Services Incorporated Mid-Career Award. MJS has received speaker-fees from Hamilton Medical. JL has received consultancy fees from Baxter and Glaxosmithkline. All other authors declare no conflict of interest.
Figures
References
-
- Thille AW, Peñuelas O, Lorente JA, Fernández-Segoviano P, Rodriguez J-M, Aramburu J-A, et al. Predictors of diffuse alveolar damage in patients with acute respiratory distress syndrome: a retrospective analysis of clinical autopsies. Crit Care Lond Engl. 2017;21:254. doi: 10.1186/s13054-017-1852-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
