

Fibroblast Activation Protein-Specific PET/CT Imaging in Fibrotic Interstitial Lung Diseases and Lung Cancer: A Translational Exploratory Study
- PMID: 34272325
- PMCID: PMC8717194
- DOI: 10.2967/jnumed.121.261925
Fibroblast Activation Protein-Specific PET/CT Imaging in Fibrotic Interstitial Lung Diseases and Lung Cancer: A Translational Exploratory Study
Abstract
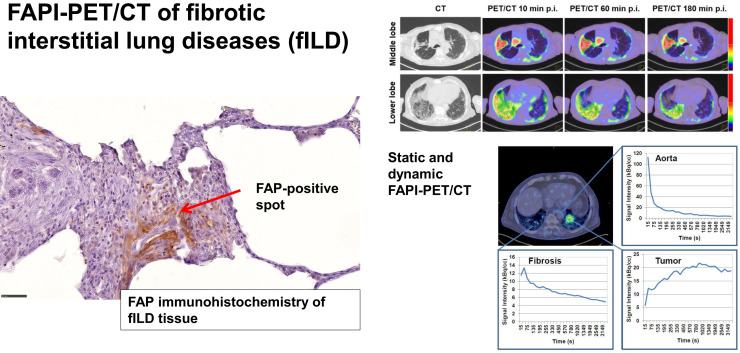
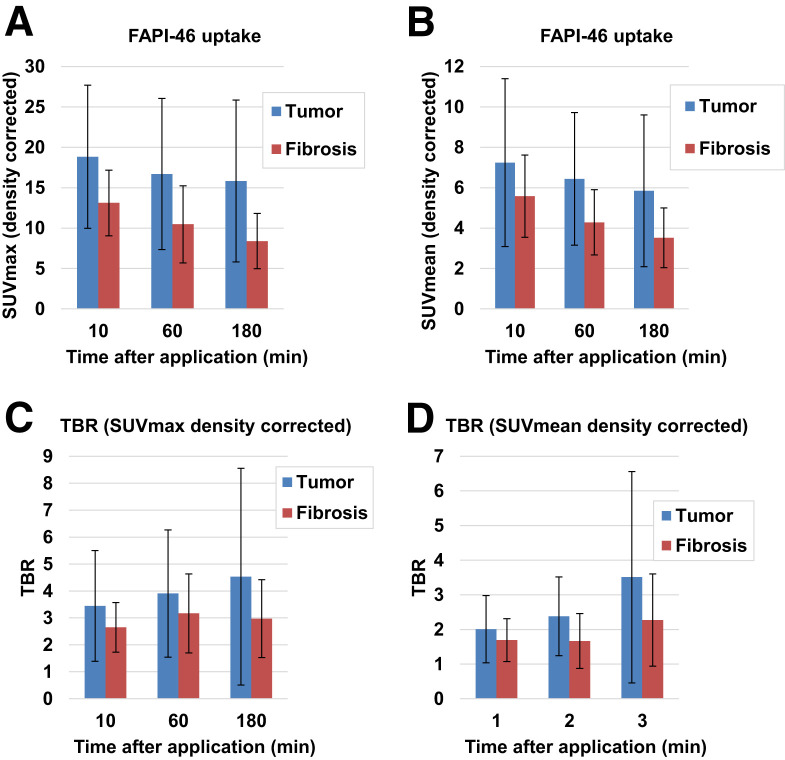
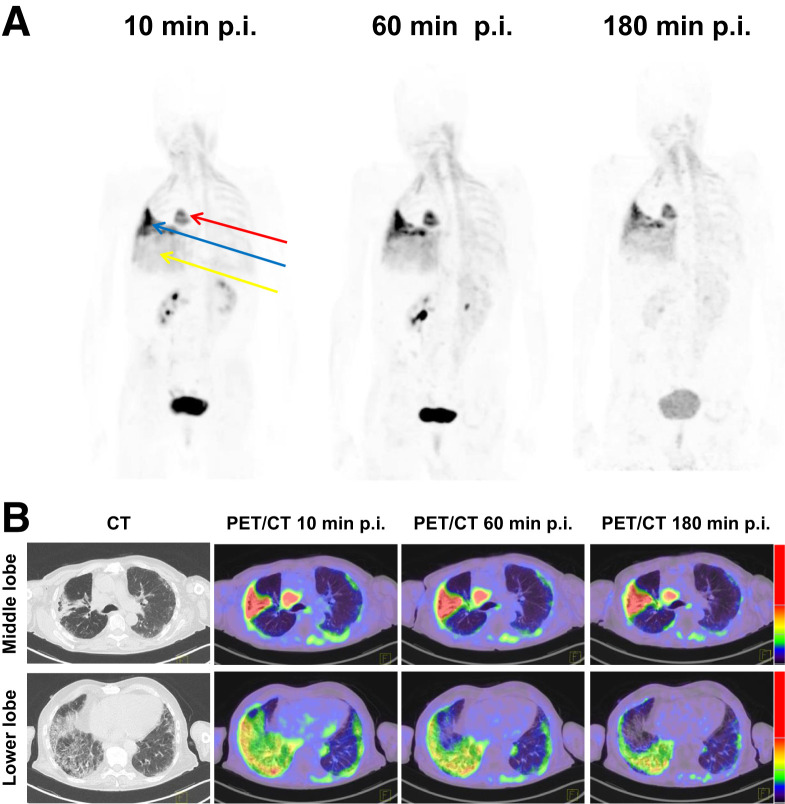
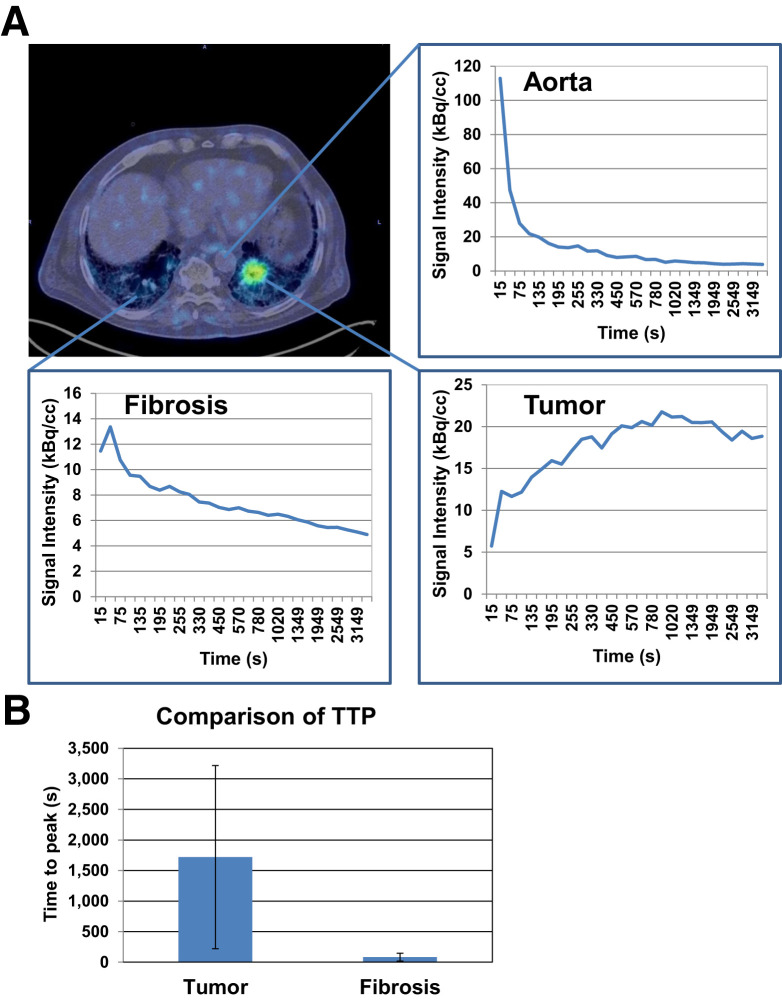
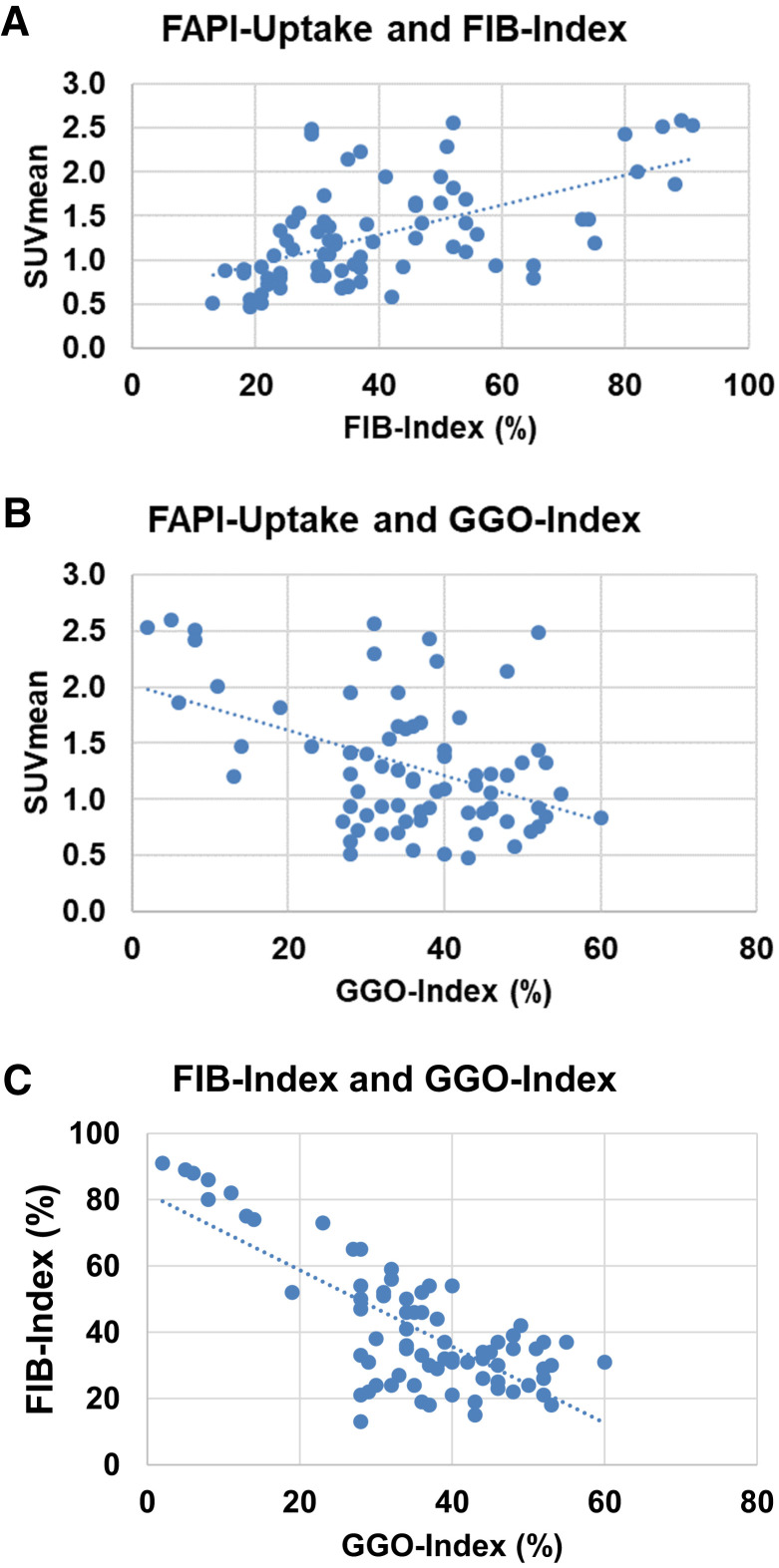
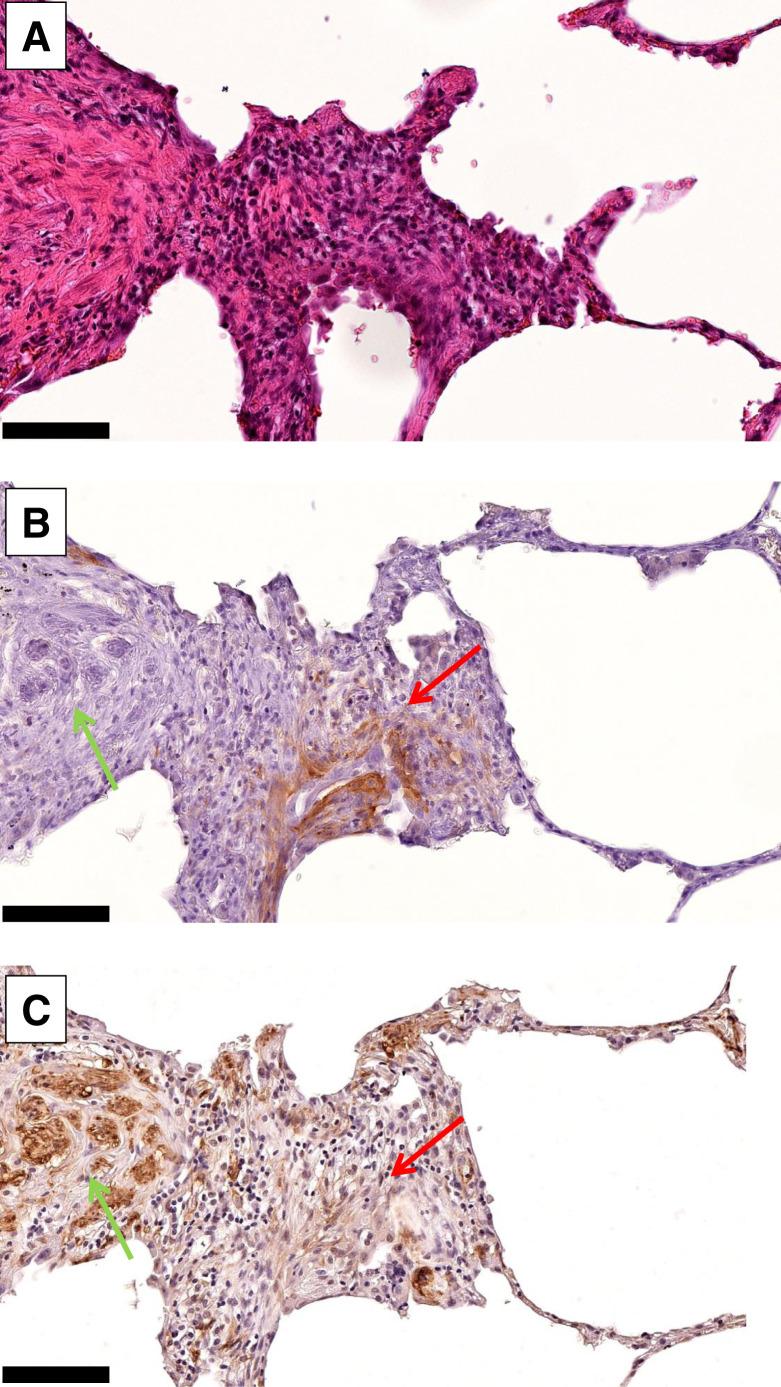
Interstitial lung diseases (ILDs) comprise over 200 parenchymal lung disorders. Among them, fibrosing ILDs, especially idiopathic pulmonary fibrosis, are associated with a poor prognosis, whereas some other ILDs, such as sarcoidosis, have a much better prognosis. A high proportion manifests as fibrotic ILD (fILD). Lung cancer (LC) is a frequent complication of fILD. Activated fibroblasts are crucial for fibrotic processes in fILD. The aim of this exploratory study was to evaluate the imaging properties of static and dynamic fibroblast activation protein (FAP) inhibitor (FAPI) PET/CT in various types of fILD and to confirm FAP expression in fILD lesions by FAP immunohistochemistry of human fILD biopsy samples and of lung sections of genetically engineered (Nedd4-2-/- ) mice with an idiopathic pulmonary fibrosislike lung disease. Methods: PET scans of 15 patients with fILD and suspected LC were acquired 10, 60, and 180 min after the administration of 150-250 MBq of a 68Ga-labeled FAPI tracer (FAPI-46). In 3 patients, dynamic scans over 40 min were performed instead of imaging after 10 min. The SUVmax and SUVmean of fibrotic lesions and LC were measured and CT-density-corrected. Target-to-background ratios (TBRs) were calculated. PET imaging was correlated with CT-based fibrosis scores. Time-activity curves derived from dynamic imaging were analyzed. FAP immunohistochemistry of 4 human fILD biopsy samples and of fibrotic lungs of Nedd4-2-/- mice was performed. Results: fILD lesions as well as LC showed markedly elevated 68Ga-FAPI uptake (density-corrected SUVmax and SUVmean 60 min after injection: 11.12 ± 6.71 and 4.29 ± 1.61, respectively, for fILD lesions and 16.69 ± 9.35 and 6.44 ± 3.29, respectively, for LC) and high TBR (TBR of density-corrected SUVmax and SUVmean 60 min after injection: 2.30 ± 1.47 and 1.67 ± 0.79, respectively, for fILD and 3.90 ± 2.36 and 2.37 ± 1.14, respectively, for LC). SUVmax and SUVmean decreased over time, with a stable TBR for fILD and a trend toward an increasing TBR in LC. Dynamic imaging showed differing time-activity curves for fILD and LC. 68Ga-FAPI uptake showed a positive correlation with the CT-based fibrosis index. Immunohistochemistry of human biopsy samples and the lungs of Nedd4-2-/- mice showed a patchy expression of FAP in fibrotic lesions, preferentially in the transition zone to healthy lung parenchyma. Conclusion:68Ga-FAPI PET/CT imaging is a promising new imaging modality for fILD and LC. Its potential clinical value for monitoring and therapy evaluation of fILD should be investigated in future studies.
Keywords: fibroblast activation protein; interstitial lung disease; lung cancer.
© 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Behr J, Prasse A, Wirtz H, et al. .Survival and course of lung function in the presence or absence of antifibrotic treatment in patients with idiopathic pulmonary fibrosis: long-term results of the INSIGHTS-IPF registry. Eur Respir J. 2020;56:1902279. - PubMed
-
- George PM, Spagnolo P, Kreuter M, et al. .Progressive fibrosing interstitial lung disease: clinical uncertainties, consensus recommendations, and research priorities. Lancet Respir Med. 2020;8:925–934. - PubMed
-
- Richeldi L, Collard HR, Jones MG. Idiopathic pulmonary fibrosis. Lancet. 2017;389:1941–1952. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous