

Improving clinical utility of GAD65 autoantibodies by electrochemiluminescence assay and clinical phenotype when identifying autoimmune adult-onset diabetes
- PMID: 34272582
- PMCID: PMC8382643
- DOI: 10.1007/s00125-021-05492-6
Improving clinical utility of GAD65 autoantibodies by electrochemiluminescence assay and clinical phenotype when identifying autoimmune adult-onset diabetes
Abstract
Aims/hypothesis: It is important to differentiate the two major phenotypes of adult-onset diabetes, autoimmune type 1 diabetes and non-autoimmune type 2 diabetes, especially as type 1 diabetes presents in adulthood. Serum GAD65 autoantibodies (GADA) are the most sensitive biomarker for adult-onset autoimmune type 1 diabetes, but the clinical value of GADA by current standard radiobinding assays (RBA) remains questionable. The present study focused on the clinical utility of GADA differentiated by a new electrochemiluminescence (ECL) assay in patients with adult-onset diabetes.
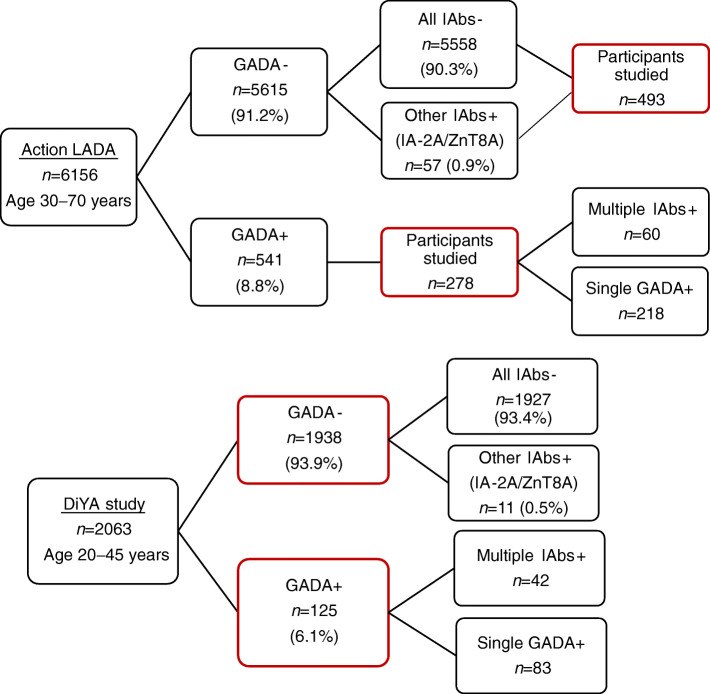
Methods: Two cohorts were analysed including 771 diabetic participants, 30-70 years old, from the Action LADA study (n = 6156), and 2063 diabetic participants, 20-45 years old, from the Diabetes in Young Adults (DiYA) study. Clinical characteristics of participants, including requirement of early insulin treatment, BMI and development of multiple islet autoantibodies, were analysed according to the status of RBA-GADA and ECL-GADA, respectively, and compared between these two assays.
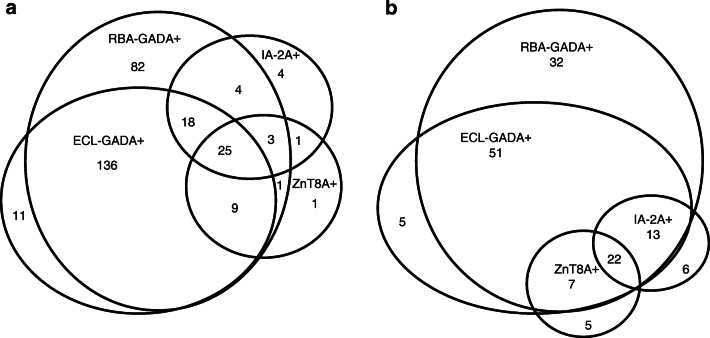
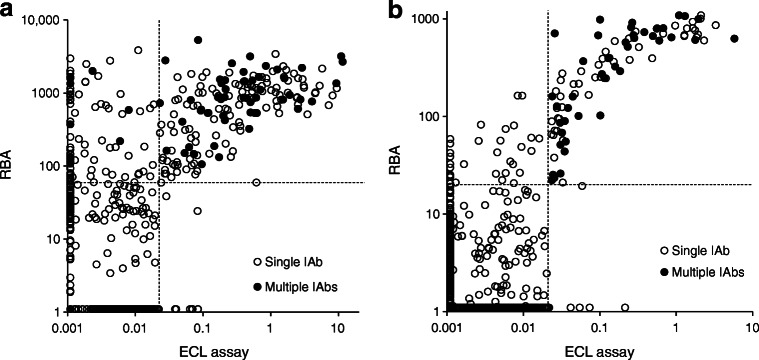
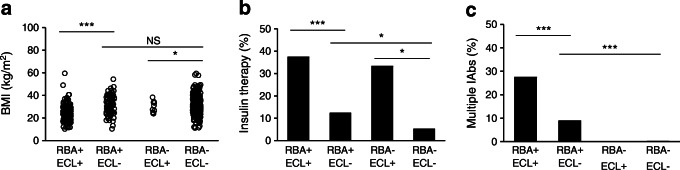
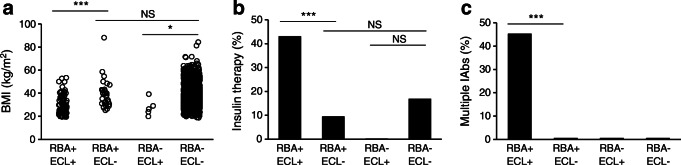
Results: GADA was the most prevalent and predominant autoantibody, >90% in both cohorts. GADA positivity by either RBA or ECL assay significantly discriminated clinical type 1 from type 2 diabetes. However, in both cohorts, participants with ECL-GADA positivity were more likely to require early insulin treatment, have multiple islet autoantibodies, and be less overweight (for all p < 0.0001). However, clinical phenotype, age at diagnosis and BMI independently improved positive predictive value (PPV) for the requirement of insulin treatment, even augmenting ECL-GADA. Participants with GADA detectable by RBA, but not confirmed by ECL, had a phenotype more similar to type 2 diabetes. These RBA-GADA positive individuals had lower affinity GADA compared with participants in which GADA was confirmed by ECL assay.
Conclusions/interpretation: Detection of GADA by ECL assay, given technical advantages over RBA-GADA, identified adult-onset diabetes patients at higher risk of requiring early insulin treatment, as did clinical phenotype, together allowing for more accurate clinical diagnosis and management.
Keywords: Adult-onset diabetes; Autoantibodies; Biomarker; ECL assay.
© 2021. The Author(s).
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
