

Indirect Comparison of Topiramate and Monoclonal Antibodies Against CGRP or Its Receptor for the Prophylaxis of Episodic Migraine: A Systematic Review with Meta-Analysis
- PMID: 34272688
- PMCID: PMC8354912
- DOI: 10.1007/s40263-021-00834-9
Indirect Comparison of Topiramate and Monoclonal Antibodies Against CGRP or Its Receptor for the Prophylaxis of Episodic Migraine: A Systematic Review with Meta-Analysis
Abstract
Background: Head-to-head comparator trials between first-line oral migraine preventatives and the new monoclonal antibodies (mAbs) blocking the calcitonin gene-related peptide (CGRP) pathway have not been published to date.
Objectives: This study aimed to indirectly compare the clinical efficacy and safety of mAbs against CGRP or its receptor (CGRPR) and topiramate in episodic migraine prophylaxis using meta-analysis.
Methods: We included controlled trials testing efficacy and safety of erenumab, galcanezumab, fremanezumab, eptinezumab, and topiramate in adults diagnosed with episodic migraine. We searched PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov from January 2000 to November 2020. We used the Risk of Bias 2 (RoB2) tool to assess the risk of bias and report pooled mean effects (mean difference and risk ratio) as estimated in a random effect model. For efficacy analysis, we determined the reduction of monthly migraine days (MMDs), reduction of days with acute medication (AMDs), and 50% responder rates (50% RR). For safety, we determined adverse events (AEs) occurring in ≥ 2% of study participants and the number of patients who discontinue treatment due to AEs (DAEs). The number needed to treat (NNT) and to harm (NNH) were estimated as well as the likelihood to help or harm (LLH).
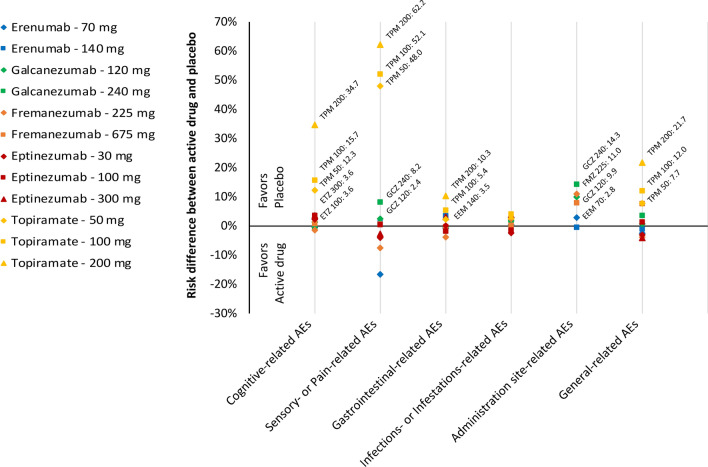
Results: We included 13 trials involving 7557 patients: three trials with erenumab, two trials with galcanezumab, two trials with fremanezumab, one trial with eptinezumab, and five trials with topiramate, for the prophylaxis of episodic migraine in adults. The placebo-subtracted reduction (pooled mean difference) of MMDs were - 1.55 (95% CI - 1.86 to - 1.24; active drug n = 3326 vs placebo n = 2219, 8 studies) for the CGRP(R) mAb and - 1.11 (95% CI - 1.62 to - 0.59; active drug n = 1032 vs placebo n = 543, 4 studies) for topiramate (p for subgroup difference = 0.15). 'Cognitive' and 'sensory & pain'-related adverse events occurred more often in patients treated with topiramate compared with those treated with a CGRP(R) mAb (p for subgroup difference 0.03 and < 0.001, respectively). Based on the 50% RR and DAE, the NNT, NNH, and LHH for the CGRP(R) mAbs were 6, 130, and 24.3:1, respectively. For topiramate, these values were 7, 9, and 1.8:1, respectively.
Conclusion: The efficacy of CGRP(R) mAbs to reduce migraine days does not differ from topiramate. However, the safety profile is in favor of the CGRP(R) mAbs, with a higher likelihood to help than to harm compared with topiramate. The diversity of endpoint determination and the heterogeneity between studies for some endpoints cause some limitations for this study.
© 2021. The Author(s).
Conflict of interest statement
LHO has nothing to disclose. BR has nothing to disclose related to the submitted work. BR reports grants from Novartis; personal fees from Novartis, TEVA, and Allergan. JM reports personal fees from Novartis, outside the submitted work. TH has nothing to disclose. LN has nothing to disclose related to the submitted work. LN reports personal fees from Novartis, Allergan, TEVA, and BIAL; personal fees from Hormosan, and Eli Lilly. UR has nothing to disclose related to the submitted work. UR reports personal fees from AbbVie, Allergan, Medscape, and StreaMedUp; personal fees and institutional fees from Amgen, Eli Lilly, and TEVA; grants, personal fees, and institutional fees from Novartis; institutional fees from Alder.
Figures


References
-
- Valery LF, Amanuel AA, Kalkidan HA, Foad A, Abdishakur MA, Semaw FA, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;2017:390. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
