

Transcriptomic signatures of tumors undergoing T cell attack
- PMID: 34272988
- PMCID: PMC10992966
- DOI: 10.1007/s00262-021-03015-1
Transcriptomic signatures of tumors undergoing T cell attack
Abstract
Background: Studying tumor cell-T cell interactions in the tumor microenvironment (TME) can elucidate tumor immune escape mechanisms and help predict responses to cancer immunotherapy.
Methods: We selected 14 pairs of highly tumor-reactive tumor-infiltrating lymphocytes (TILs) and autologous short-term cultured cell lines, covering four distinct tumor types, and co-cultured TILs and tumors at sub-lethal ratios in vitro to mimic the interactions occurring in the TME. We extracted gene signatures associated with a tumor-directed T cell attack based on transcriptomic data of tumor cells.
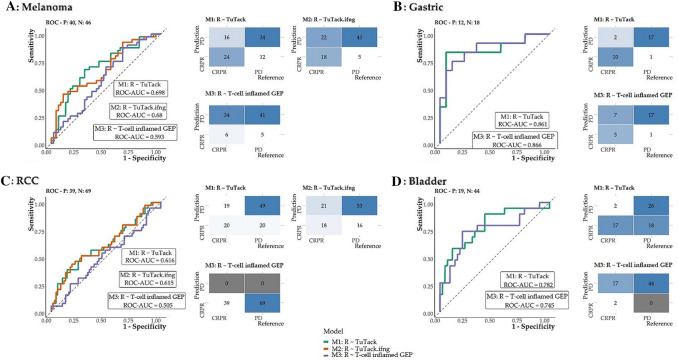
Results: An autologous T cell attack induced pronounced transcriptomic changes in the attacked tumor cells, partially independent of IFN-γ signaling. Transcriptomic changes were mostly independent of the tumor histological type and allowed identifying common gene expression changes, including a shared gene set of 55 transcripts influenced by T cell recognition (Tumors undergoing T cell attack, or TuTack, focused gene set). TuTack scores, calculated from tumor biopsies, predicted the clinical outcome after anti-PD-1/anti-PD-L1 therapy in multiple tumor histologies. Notably, the TuTack scores did not correlate to the tumor mutational burden, indicating that these two biomarkers measure distinct biological phenomena.
Conclusions: The TuTack scores measure the effects on tumor cells of an anti-tumor immune response and represent a comprehensive method to identify immunologically responsive tumors. Our findings suggest that TuTack may allow patient selection in immunotherapy clinical trials and warrant its application in multimodal biomarker strategies.
Keywords: Adaptive immune resistance; Anti-PD-1; Anti-PD-L1; Immunotherapy biomarkers; Patient selection; Transcriptomics.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
MD has received honoraria for lectures from Roche and Novartis (past two years). IMS has received honoraria for consultancies and lectures from Novartis, Roche, Merck and Bristol-Myers Squibb; a restricted research grant from Novartis; and financial support for attending symposia from Bristol-Myers Squibb, Merck, Novartis, Pfizer and Roche. A patent (inventors AG, AS and MD) disclosing methods to predict response to immunotherapy has been submitted. The rights of the patent applications will be transferred to Capital Region of Denmark, according to the Danish Law of Public Inventions at Public Research Institutions. All other authors declare that they have no conflict of interest.
Figures



References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
