

Current and emerging drug targets in heart failure treatment
- PMID: 34273070
- PMCID: PMC9197912
- DOI: 10.1007/s10741-021-10137-2
Current and emerging drug targets in heart failure treatment
Abstract
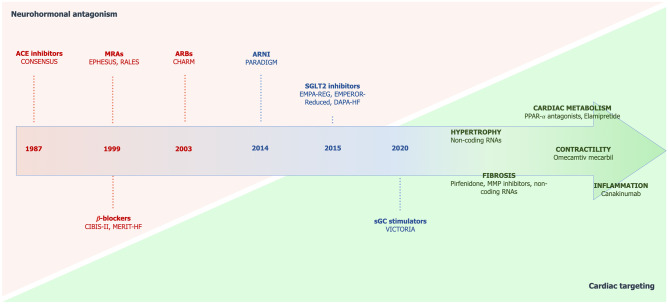
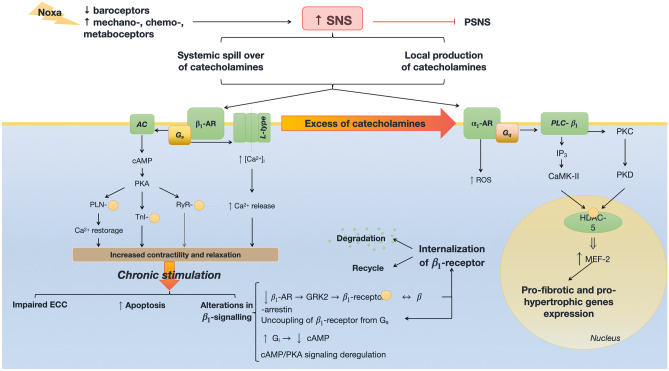
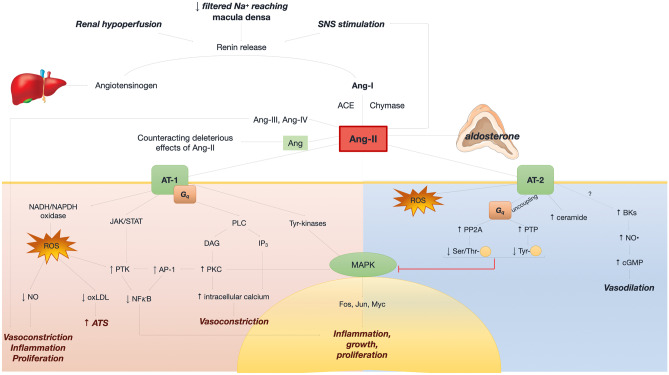
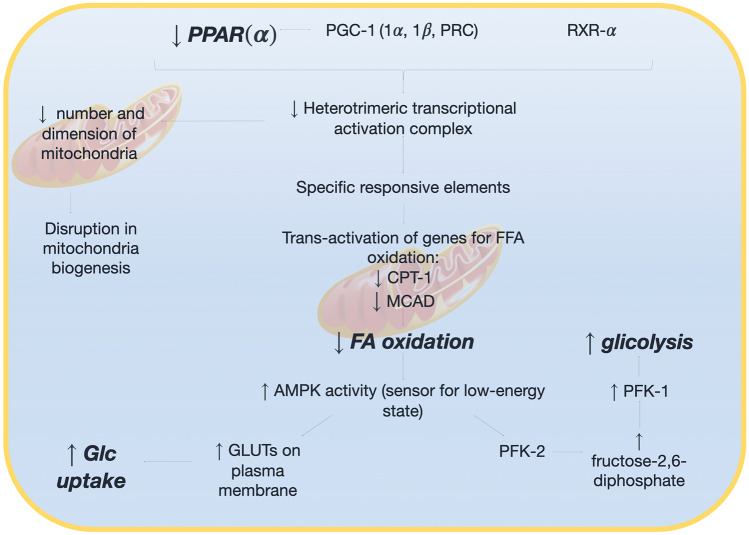
After initial strategies targeting inotropism and congestion, the neurohormonal interpretative model of heart failure (HF) pathophysiology has set the basis for current pharmacological management of HF, as most of guideline recommended drug classes, including beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and mineralocorticoid receptor antagonists, blunt the activation of detrimental neurohormonal axes, namely sympathetic and renin-angiotensin-aldosterone (RAAS) systems. More recently, sacubitril/valsartan, a first-in-class angiotensin receptor neprilysin inhibitor, combining inhibition of RAAS and potentiation of the counter-regulatory natriuretic peptide system, has been consistently demonstrated to reduce mortality and HF-related hospitalization. A number of novel pharmacological approaches have been tested during the latest years, leading to mixed results. Among them, drugs acting directly at a second messenger level, such as the soluble guanylate cyclase stimulator vericiguat, or other addressing myocardial energetics and mitochondrial function, such as elamipretide or omecamtiv-mecarbil, will likely change the therapeutic management of patients with HF. Sodium glucose cotransporter 2 inhibitors, initially designed for the management of type 2 diabetes mellitus, have been recently demonstrated to improve outcome in HF, although mechanisms of their action on cardiovascular system are yet to be elucidated. Most of these emerging approaches have shifted the therapeutic target from neurohormonal systems to the heart, by improving cardiac contractility, metabolism, fibrosis, inflammation, and remodeling. In the present paper, we review from a pathophysiological perspective current and novel therapeutic strategies in chronic HF.
Keywords: Emerging targets; Heart failure; Neurohormonal antagonism; Pharmacodynamics; Pharmacotherapy; SGLT2 inhibitors.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Maggioni AP, Dahlström U, Filippatos G, et al (2013) EURObservational research programme: Regional differences and 1-year follow-up results of the heart failure pilot survey (ESC-HF Pilot). Eur J Heart Fail. 15:808–817. 10.1093/eurjhf/hft050 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
