

Availability of facility resources and services and infection-related maternal outcomes in the WHO Global Maternal Sepsis Study: a cross-sectional study
- PMID: 34273300
- PMCID: PMC8370881
- DOI: 10.1016/S2214-109X(21)00248-5
Availability of facility resources and services and infection-related maternal outcomes in the WHO Global Maternal Sepsis Study: a cross-sectional study
Abstract
Background: Infections are among the leading causes of maternal mortality and morbidity. The Global Maternal Sepsis and Neonatal Initiative, launched in 2016 by WHO and partners, sought to reduce the burden of maternal infections and sepsis and was the basis upon which the Global Maternal Sepsis Study (GLOSS) was implemented in 2017. In this Article, we aimed to describe the availability of facility resources and services and to analyse their association with maternal outcomes.
Methods: GLOSS was a facility-based, prospective, 1-week inception cohort study implemented in 713 health-care facilities in 52 countries and included 2850 hospitalised pregnant or recently pregnant women with suspected or confirmed infections. All women admitted for or in hospital with suspected or confirmed infections during pregnancy, childbirth, post partum, or post abortion at any of the participating facilities between Nov 28 and Dec 4 were eligible for inclusion. In this study, we included all GLOSS participating facilities that collected facility-level data (446 of 713 facilities). We used data obtained from individual forms completed for each enrolled woman and their newborn babies by trained researchers who checked the medical records and from facility forms completed by hospital administrators for each participating facility. We described facilities according to country income level, compliance with providing core clinical interventions and services according to women's needs and reported availability, and severity of infection-related maternal outcomes. We used a logistic multilevel mixed model for assessing the association between facility characteristics and infection-related maternal outcomes.
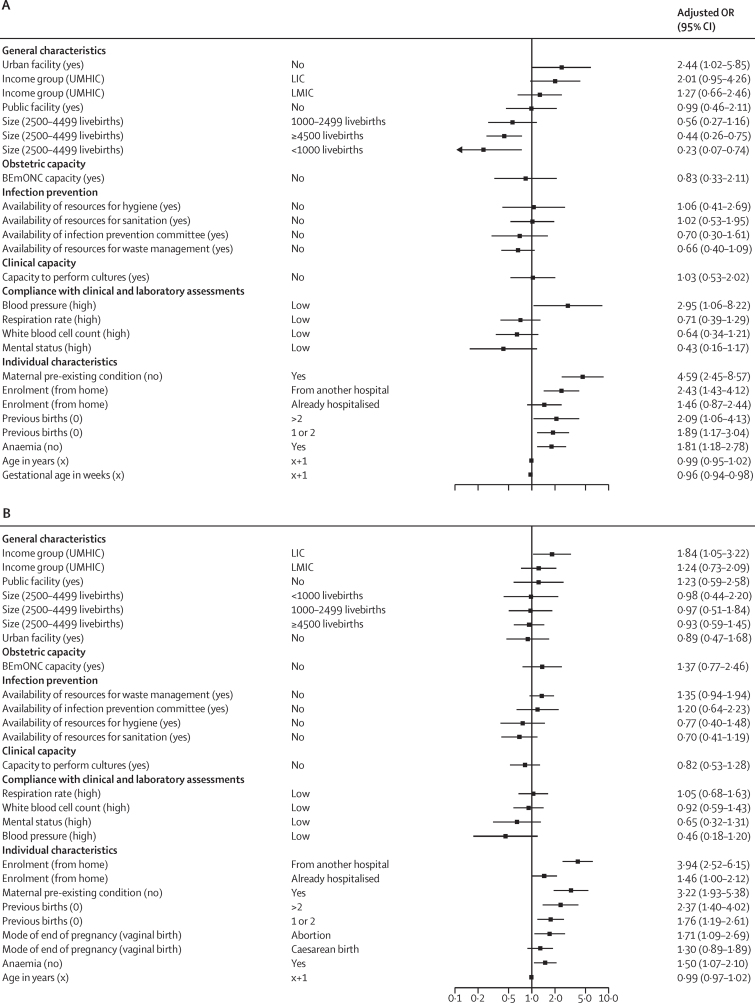
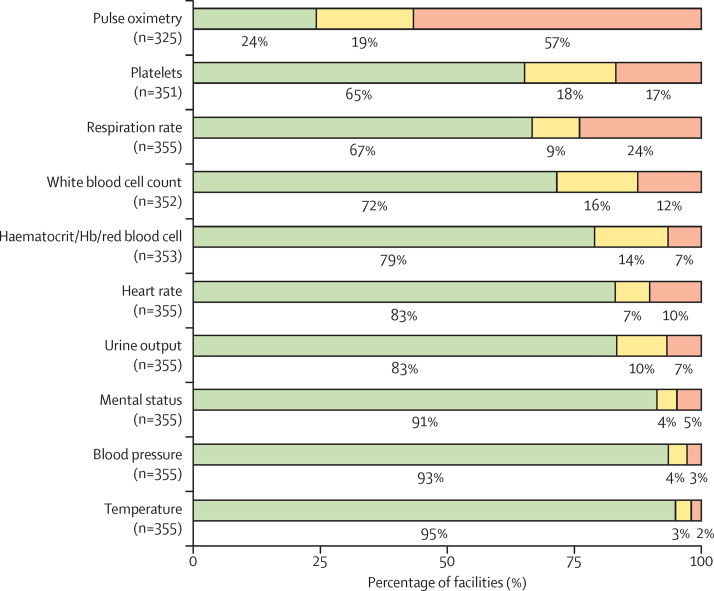
Findings: We included 446 facilities from 46 countries that enrolled 2560 women. We found a high availability of most services and resources needed for obstetric care and infection prevention. We found increased odds for severe maternal outcomes among women enrolled during the post-partum or post-abortion period from facilities located in low-income countries (adjusted odds ratio 1·84 [95% CI 1·05-3·22]) and among women enrolled during pregnancy or childbirth from non-urban facilities (adjusted odds ratio 2·44 [1·02-5·85]). Despite compliance being high overall, it was low with regards to measuring respiratory rate (85 [24%] of 355 facilities) and measuring pulse oximetry (184 [57%] of 325 facilities).
Interpretation: While health-care facilities caring for pregnant and recently pregnant women with suspected or confirmed infections have access to a wide range of resources and interventions, worse maternal outcomes are seen among recently pregnant women located in low-income countries than among those in higher-income countries; this trend is similar for pregnant women. Compliance with cost-effective clinical practices and timely care of women with particular individual characteristics can potentially improve infection-related maternal outcomes.
Funding: UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, WHO, Merck for Mothers, and US Agency for International Development.
© 2021 World Health Organization; licensee Elsevier. This is an Open Access article under the CC BY 3.0 IGO license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products, or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Surviving maternal sepsis in low-income countries.Lancet Glob Health. 2021 Sep;9(9):e1183-e1184. doi: 10.1016/S2214-109X(21)00294-1. Epub 2021 Jul 21. Lancet Glob Health. 2021. PMID: 34273301 No abstract available.
References
-
- Campbell OM, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368:1284–1299. - PubMed
-
- WHO. UNICEF. UNFPA. World Bank Group. UN Population Division . World Health Organization; Geneva, Switzerland: 2019. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.
-
- Say L, Chou D, Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
-
- Global Maternal and Neonatal Sepsis Initiative Working Group The Global Maternal and Neonatal Sepsis Initiative. a call for collaboration and action by 2030. Lancet Glob Health. 2017;5:e390–e391. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
