

Characterisation of in-hospital complications associated with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol UK: a prospective, multicentre cohort study
- PMID: 34274064
- PMCID: PMC8285118
- DOI: 10.1016/S0140-6736(21)00799-6
Characterisation of in-hospital complications associated with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol UK: a prospective, multicentre cohort study
Erratum in
-
Department of Error.Lancet. 2021 Jul 31;398(10298):390. doi: 10.1016/S0140-6736(21)01690-1. Lancet. 2021. PMID: 34332681 Free PMC article. No abstract available.
Abstract
Background: COVID-19 is a multisystem disease and patients who survive might have in-hospital complications. These complications are likely to have important short-term and long-term consequences for patients, health-care utilisation, health-care system preparedness, and society amidst the ongoing COVID-19 pandemic. Our aim was to characterise the extent and effect of COVID-19 complications, particularly in those who survive, using the International Severe Acute Respiratory and Emerging Infections Consortium WHO Clinical Characterisation Protocol UK.
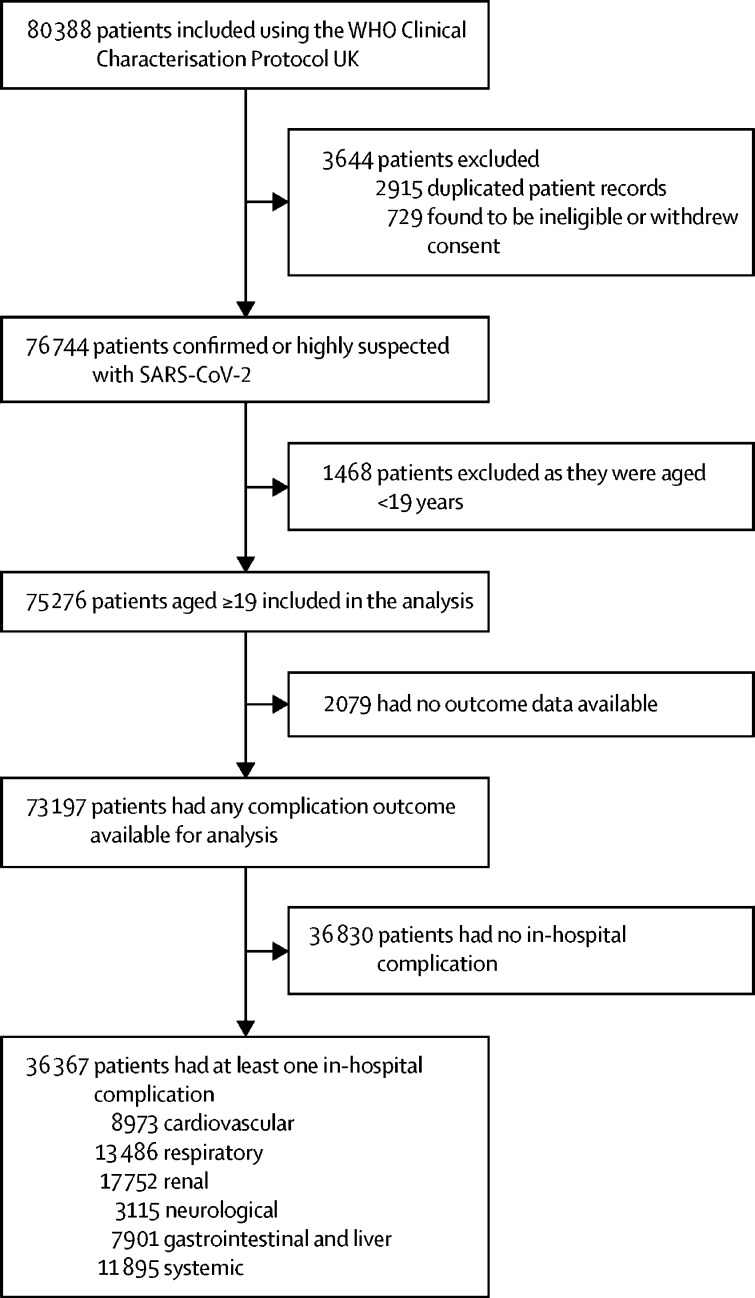
Methods: We did a prospective, multicentre cohort study in 302 UK health-care facilities. Adult patients aged 19 years or older, with confirmed or highly suspected SARS-CoV-2 infection leading to COVID-19 were included in the study. The primary outcome of this study was the incidence of in-hospital complications, defined as organ-specific diagnoses occurring alone or in addition to any hallmarks of COVID-19 illness. We used multilevel logistic regression and survival models to explore associations between these outcomes and in-hospital complications, age, and pre-existing comorbidities.
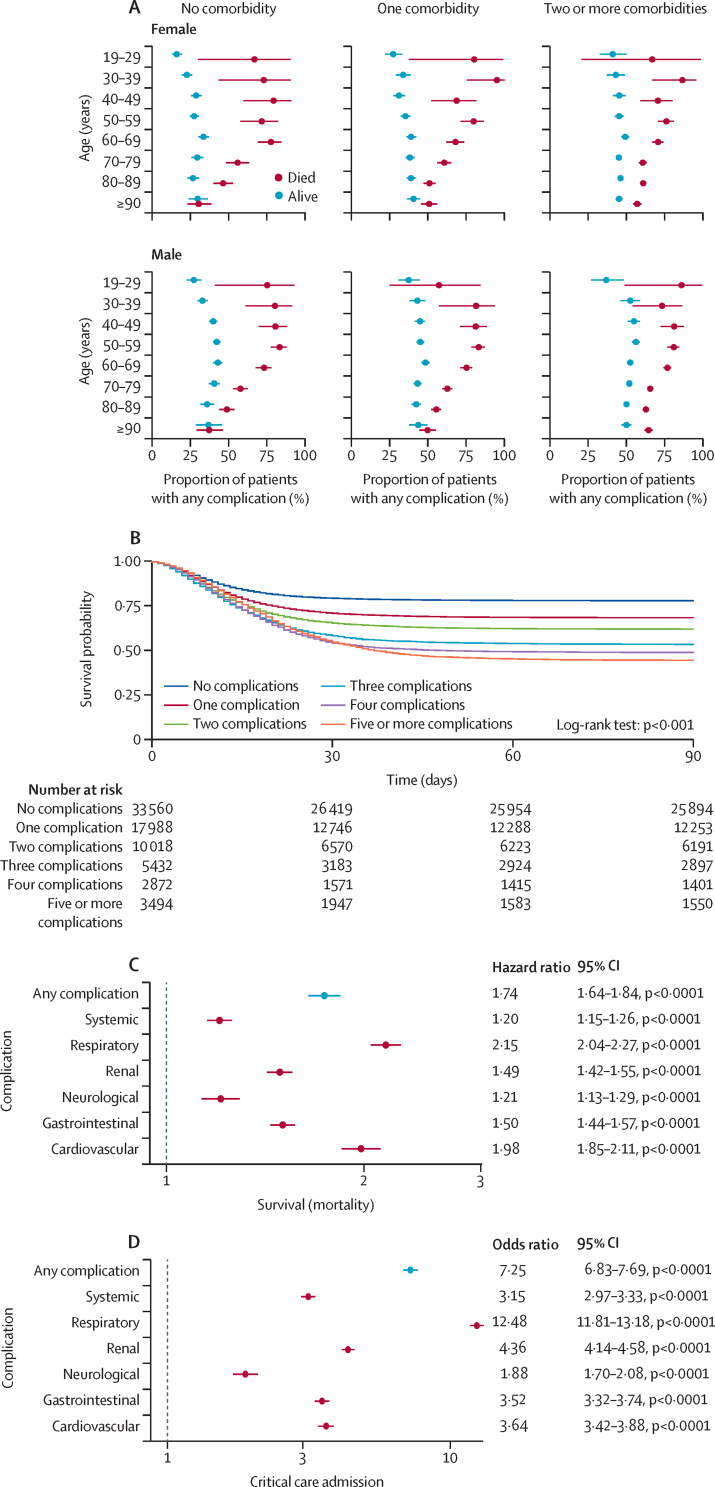
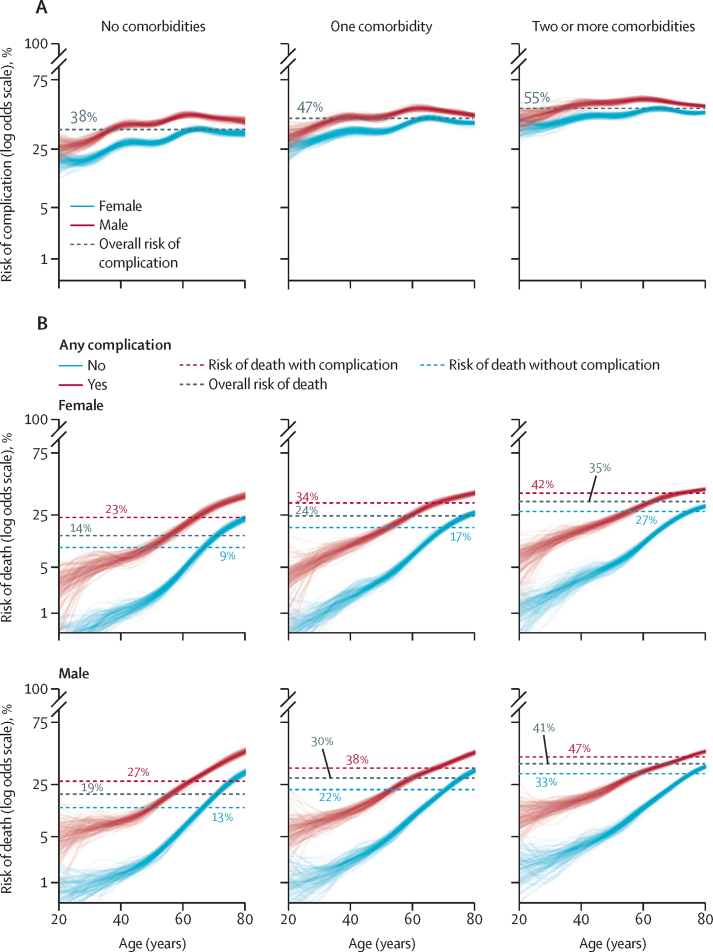
Findings: Between Jan 17 and Aug 4, 2020, 80 388 patients were included in the study. Of the patients admitted to hospital for management of COVID-19, 49·7% (36 367 of 73 197) had at least one complication. The mean age of our cohort was 71·1 years (SD 18·7), with 56·0% (41 025 of 73 197) being male and 81·0% (59 289 of 73 197) having at least one comorbidity. Males and those aged older than 60 years were most likely to have a complication (aged ≥60 years: 54·5% [16 579 of 30 416] in males and 48·2% [11 707 of 24 288] in females; aged <60 years: 48·8% [5179 of 10 609] in males and 36·6% [2814 of 7689] in females). Renal (24·3%, 17 752 of 73 197), complex respiratory (18·4%, 13 486 of 73 197), and systemic (16·3%, 11 895 of 73 197) complications were the most frequent. Cardiovascular (12·3%, 8973 of 73 197), neurological (4·3%, 3115 of 73 197), and gastrointestinal or liver (0·8%, 7901 of 73 197) complications were also reported.
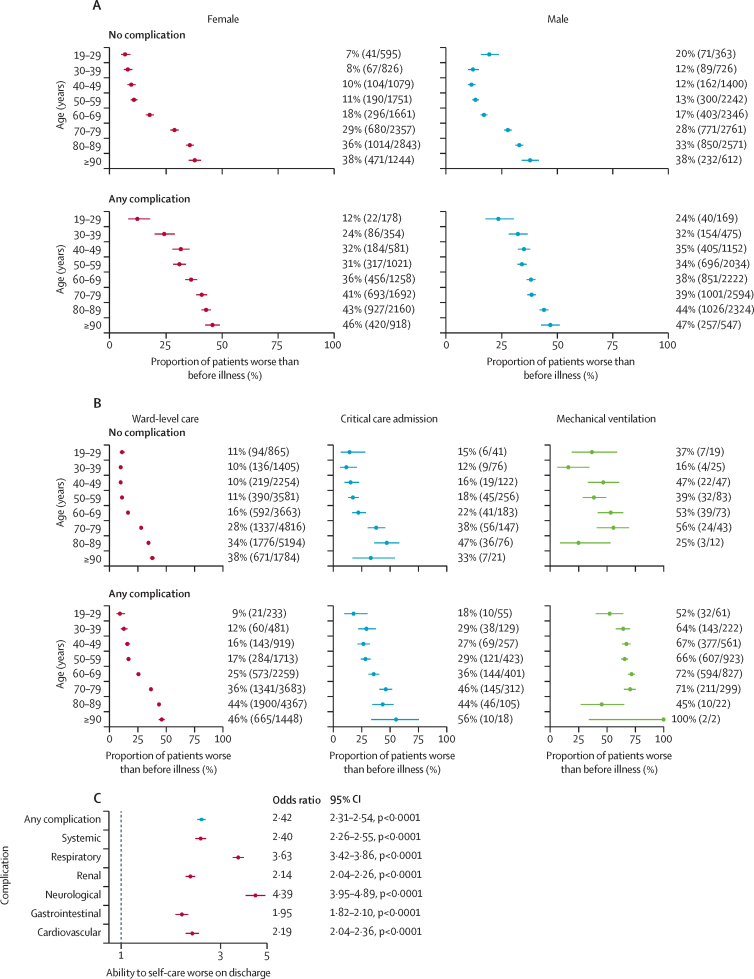
Interpretation: Complications and worse functional outcomes in patients admitted to hospital with COVID-19 are high, even in young, previously healthy individuals. Acute complications are associated with reduced ability to self-care at discharge, with neurological complications being associated with the worst functional outcomes. COVID-19 complications are likely to cause a substantial strain on health and social care in the coming years. These data will help in the design and provision of services aimed at the post-hospitalisation care of patients with COVID-19.
Funding: National Institute for Health Research and the UK Medical Research Council.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ABD reports grants from the Department of Health and Social Care (DHSC), during the conduct of the study; and grants from Wellcome Trust, outside the submitted work. PJMO reports institutional fees from consultancies from Janssen, Oxford Immunotech, Nestle, Pfizer, and the European Respiratory Society; grants from the MRC, MRC Global Challenge Research Fund, EU, NIHR Biomedical Research Centre, MRC, GlaxoSmithKline, Wellcome Trust, and NIHR Health Protection Research Unit (HPRU) in Respiratory Infection; and is NIHR senior investigator outside the submitted work. PJMO's role as president of the British Society for Immunology was unpaid but travel and accommodation at some meetings was provided by the Society.JKB reports grants from MRC UK. MGS reports grants from DHSC, NIHR UK, MRC UK, HPRU in Emerging and Zoonotic Infections, and University of Liverpool, during the conduct of the study; and is chair of the Infectious Diseases Science Advisory Board and minority shareholder of Integrum Scientific, Greensboro NC, outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
In-hospital complications associated with COVID-19.Lancet. 2021 Jul 17;398(10296):188-190. doi: 10.1016/S0140-6736(21)00983-1. Lancet. 2021. PMID: 34274053 Free PMC article. No abstract available.
References
-
- Needham DM, Feldman DR, Kho ME. The functional costs of ICU survivorship. Collaborating to improve post-ICU disability. Am J Respir Crit Care Med. 2011;183:962–964. - PubMed
Publication types
MeSH terms
Grants and funding
- MC_UU_12014/8/MRC_/Medical Research Council/United Kingdom
- MR/S032304/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12014/12/MRC_/Medical Research Council/United Kingdom
- G0701652/MRC_/Medical Research Council/United Kingdom
- MC_UU_12014/10/MRC_/Medical Research Council/United Kingdom
- MC_PC_19026/MRC_/Medical Research Council/United Kingdom
- MR/V001671/1/MRC_/Medical Research Council/United Kingdom
- 205228/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- MC_UU_12014/9/MRC_/Medical Research Council/United Kingdom
- FS/18/13/33281/BHF_/British Heart Foundation/United Kingdom
- MC_PC_19025/MRC_/Medical Research Council/United Kingdom
- MC_PC_15001/MRC_/Medical Research Council/United Kingdom
- 215091/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- 109965/Z/15/Z/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
