

Diagnostic dilemma of Hodgkin's lymphoma versus tuberculosis: a case report and review of the literature
- PMID: 34275479
- PMCID: PMC8287740
- DOI: 10.1186/s13256-021-02927-x
Diagnostic dilemma of Hodgkin's lymphoma versus tuberculosis: a case report and review of the literature
Abstract
Background: Hodgkin's Lymphoma (HL) is a rare malignancy characterised histologically by the presence of Reed-Sternberg cells. Diagnosis of lymphomas can be difficult due to broad, non-specific presentations of disease, which can be similar to several other conditions ranging from infective, inflammatory or malignant causes, with one of the most common differentials being tuberculosis (TB). We aim to highlight the diagnostic dilemma of TB versus lymphoma with an atypical presentation of HL and explored areas for further research and improvement with a non-systematic literature review using MEDLINE database and Google Scholar. Written consent was obtained from the patient in compliance with ethical guidelines.
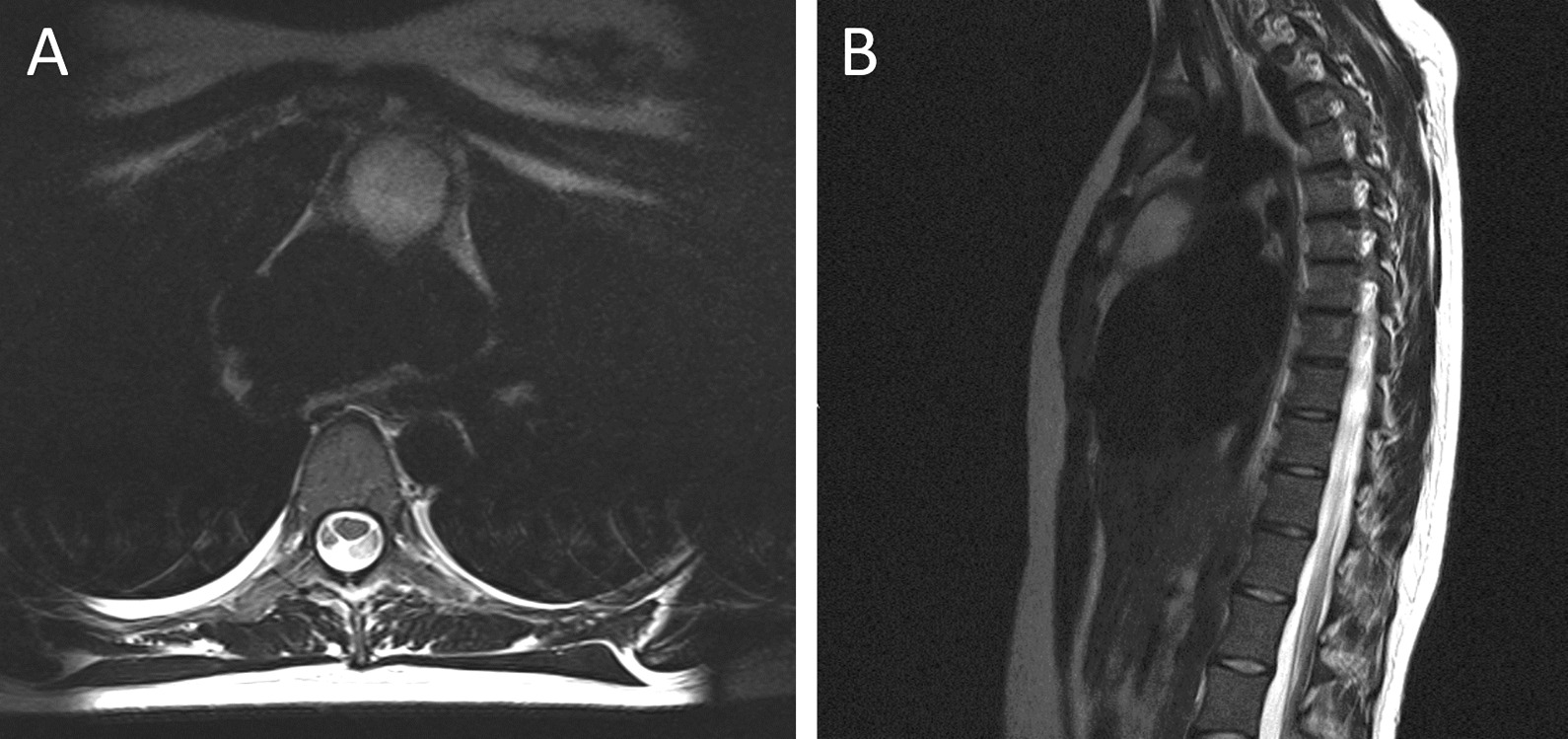
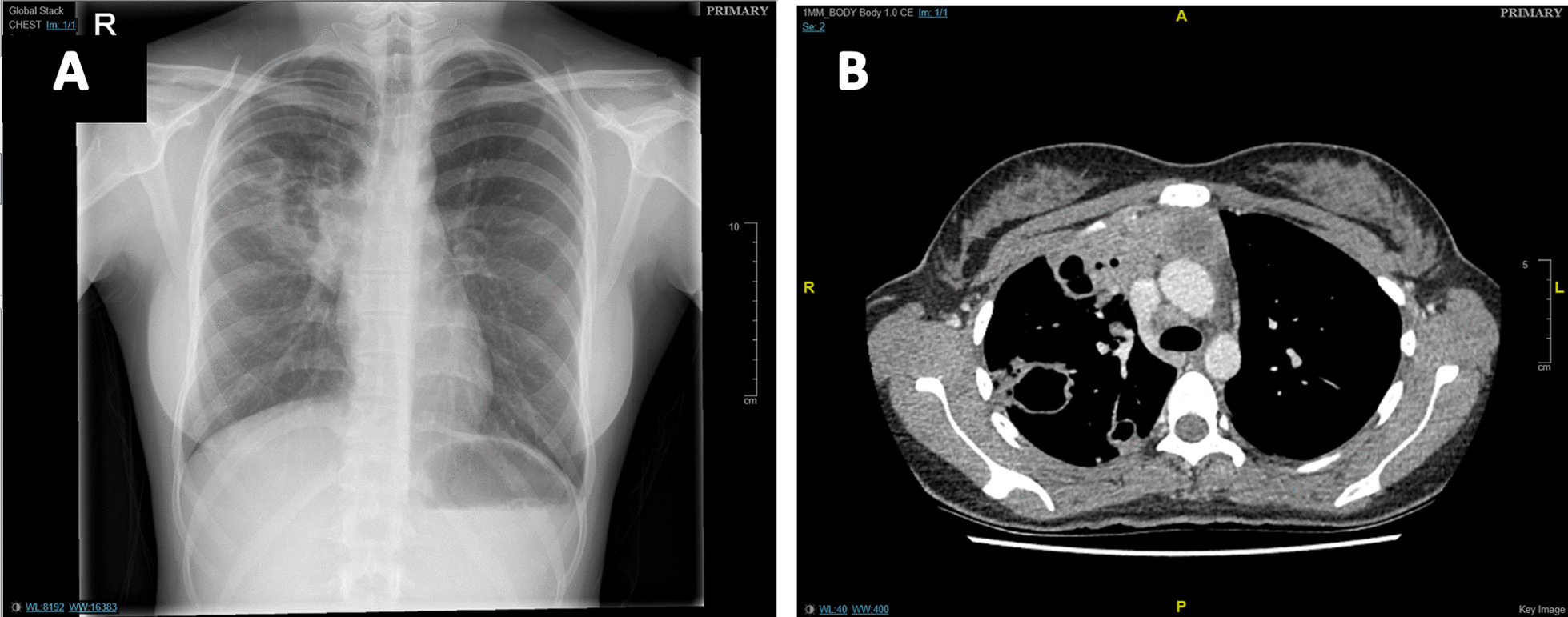
Case presentation: A 23-year-old Asian female initially presented to rheumatology with over a one-year history of neuropathic pain, alongside abnormal white cell count and inflammatory markers. This was investigated with magnetic resonance imaging resulting in an incidental finding of mediastinal mass and pulmonary infiltrates. An initial diagnosis of TB was made despite testing negative for acid-fast bacilli and anti-tubercular treatment was commenced. Four months later, following clinical deterioration and further investigations, a mediastinal biopsy assisted in diagnosing Stage IV HL.
Conclusions: Lymphoma is often misdiagnosed as TB, prolonging time to treatment and may adversely impact patient prognosis due to disease progression. Existing TB guidelines for smear-negative cases are not clear when to consider alternative diagnoses. In smear-negative TB, lymphoma should be considered as a differential and definitive diagnostic tests such as molecular testing and histological examination of biopsies should be considered earlier in the diagnostic work-up to prevent diagnostic delay.
Keywords: Case report; Diagnostic delay; Guidelines; Hodgkin’s lymphoma; Literature review; Tuberculosis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing of interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
