

Global, Regional, and National Burden of Diabetes-Related Chronic Kidney Disease From 1990 to 2019
- PMID: 34276558
- PMCID: PMC8281340
- DOI: 10.3389/fendo.2021.672350
Global, Regional, and National Burden of Diabetes-Related Chronic Kidney Disease From 1990 to 2019
Abstract
Background: Chronic kidney disease (CKD) is a public health problem largely caused by diabetes. The epidemiology of diabetes mellitus-related CKD (CKD-DM) could provide specific support to lessen global, regional, and national CKD burden.
Methods: Data were derived from the GBD 2019 study, including four measures and age-standardized rates (ASRs). Estimated annual percentage changes and 95% CIs were calculated to evaluate the variation trend of ASRs.
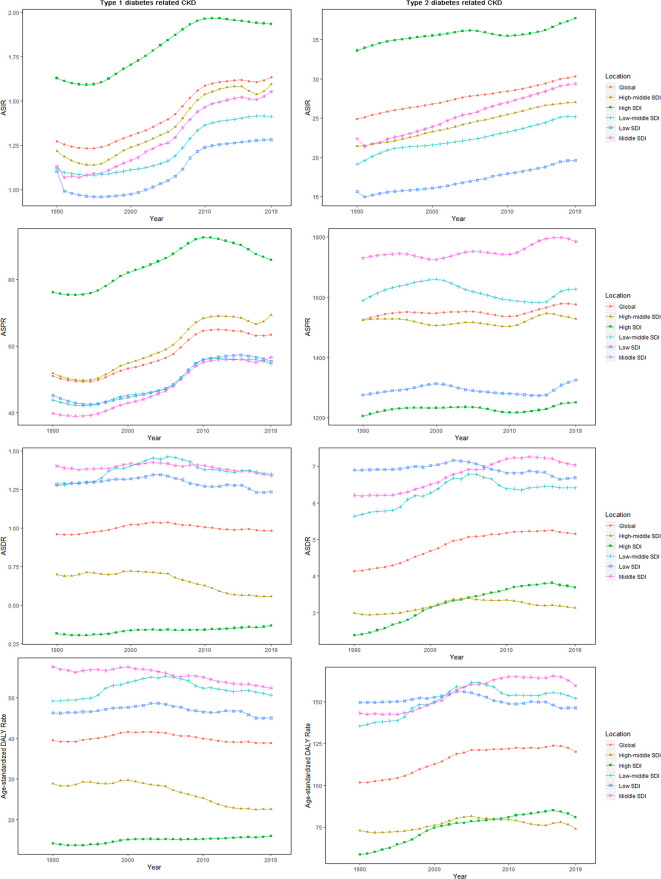
Results: Diabetes caused the majority of new cases and patients with CKD in all regions. All ASRs for type 2 diabetes-related CKD increased over 30 years. Asia and Middle socio-demographic index (SDI) quintile always carried the heaviest burden of CKD-DM. Diabetes type 2 became the second leading cause of CKD and CKD-related death and the third leading cause of CKD-related DALYs in 2019. Type 2 diabetes-related CKD accounted for most of the CKD-DM disease burden. There were 2.62 million incident cases, 134.58 million patients, 405.99 thousand deaths, and 13.09 million disability-adjusted life-years (DALYs) of CKD-DM worldwide in 2019. Age-standardized incidence (ASIR) and prevalence rate (ASPR) of type 1 diabetes-related CKD increased, whereas age-standardized death rate (ASDR) and DALY rate decreased for females and increased for males. In high SDI quintile, ASIR and ASPR of type 1 diabetes-related CKD remained the highest, with the slowest increase, whereas the ASDR and age-standardized DALY rate remained the lowest there. In high SDI quintile, ASIR of type 2 diabetes-related CKD was the highest, with the lowest increasing rate. In addition, type 2 diabetes-related CKD occurred most in people aged 80-plus years worldwide. The main age of type 2 diabetes-related CKD patients was 55-64 years in Asia and Africa. The prevalence, mortality, and DALY rate of type 2 diabetes-related CKD increased with age. As for incidence, there was a peak at 80 years, and after age of 80, the incidence declined. CKD-DM-related anemia was mainly in mild to moderate grade.
Conclusions: Increasing burden of CKD-DM varied among regions and countries. Prevention and treatment measures should be strengthened according to CKD-DM epidemiology, especially in middle SDI quintile and Asia.
Keywords: diabetes-related chronic kidney disease; disability-adjusted life-years; incidence; mortality; prevalence.
Copyright © 2021 Deng, Li, Wu, Wang, Yang, Zheng, Deng, Xiang, Zhu, Xu, Zhai, Zhang, Dai and Gao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived With Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet (Lond Engl) (2018) 392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- GBD 2017 DALYs and HALE Collaborators. Global, Regional, and National Disability-Adjusted Life-Years (DALYs) for 359 Diseases and Injuries and Healthy Life Expectancy (HALE) for 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet (Lond Engl) (2018) 392:1859–922. 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical