

Dysregulation of the Immune Environment in the Airways During HIV Infection
- PMID: 34276702
- PMCID: PMC8278481
- DOI: 10.3389/fimmu.2021.707355
Dysregulation of the Immune Environment in the Airways During HIV Infection
Abstract
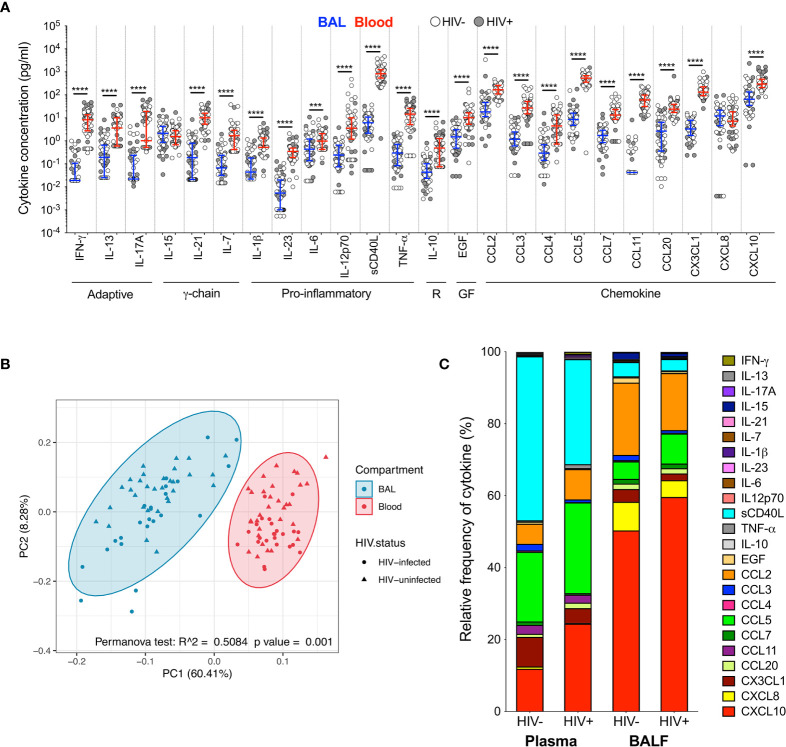
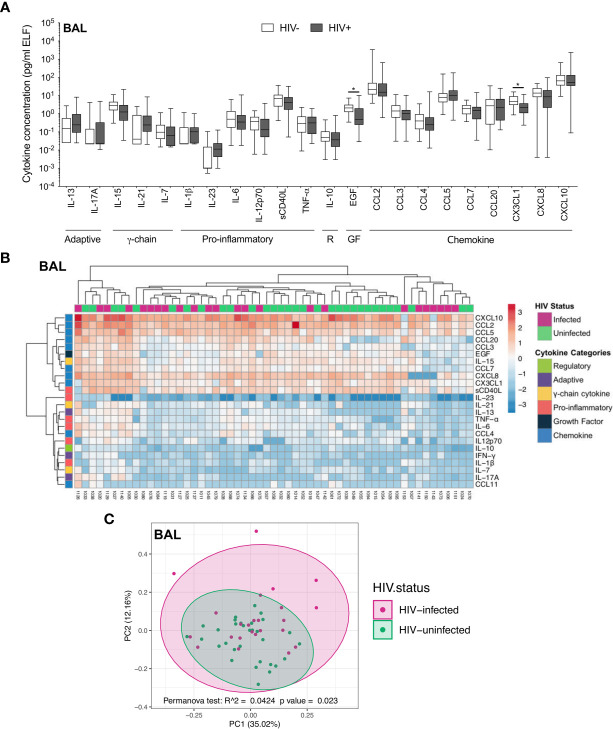
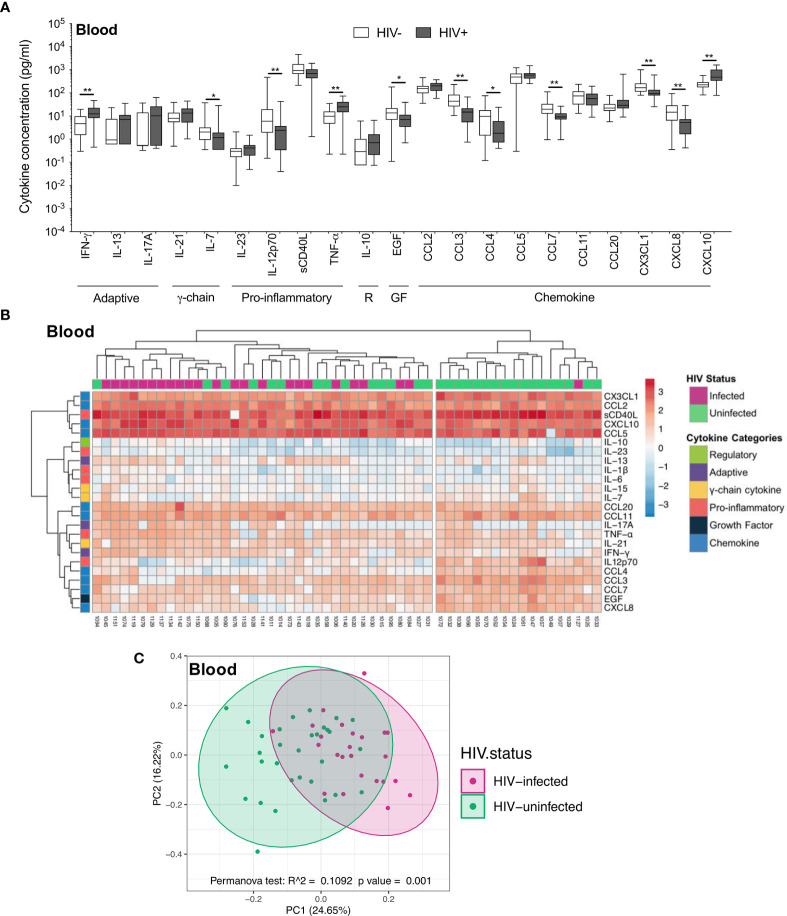
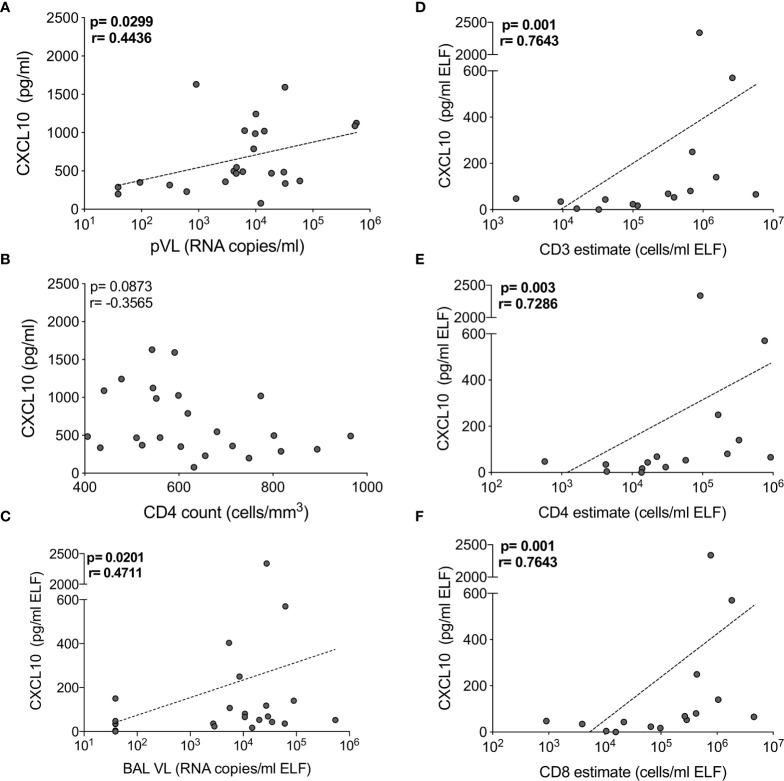
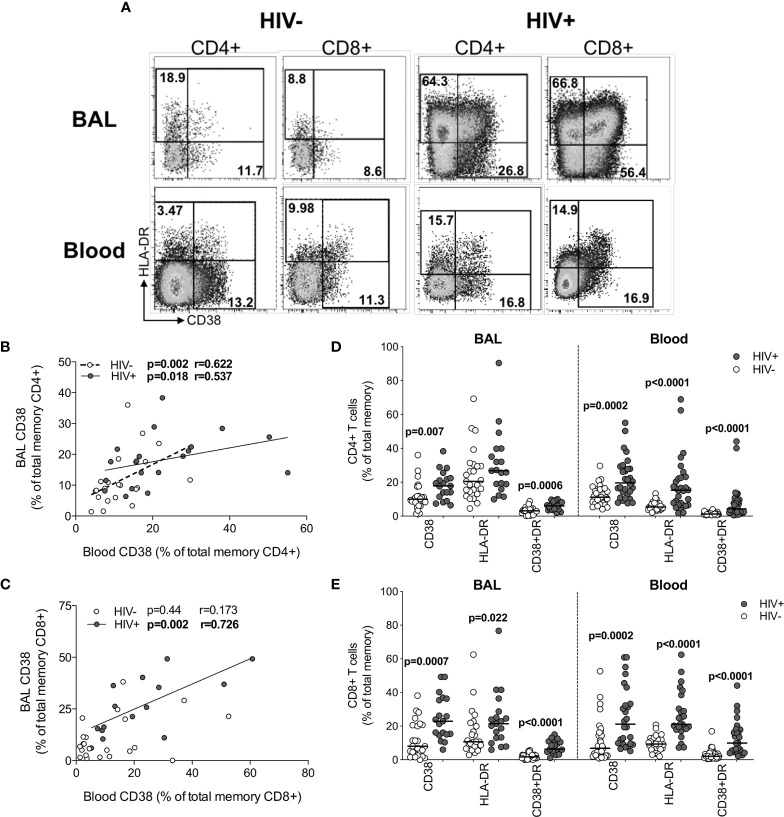
HIV-1 increases susceptibility to pulmonary infection and disease, suggesting pathogenesis in the lung. However, the lung immune environment during HIV infection remains poorly characterized. This study examined T cell activation and the cytokine milieu in paired bronchoalveolar lavage (BAL) and blood from 36 HIV-uninfected and 32 HIV-infected participants. Concentrations of 27 cytokines were measured by Luminex, and T cells were phenotyped by flow cytometry. Blood and BAL had distinct cytokine profiles (p=0.001). In plasma, concentrations of inflammatory cytokines like IFN-γ (p=0.004) and TNF-α (p=0.004) were elevated during HIV infection, as expected. Conversely, BAL cytokine concentrations were similar in HIV-infected and uninfected individuals, despite high BAL viral loads (VL; median 48,000 copies/ml epithelial lining fluid). HIV-infected individuals had greater numbers of T cells in BAL compared to uninfected individuals (p=0.007); and BAL VL positively associated with CD4+ and CD8+ T cell numbers (p=0.006 and p=0.0002, respectively) and CXCL10 concentrations (p=0.02). BAL T cells were highly activated in HIV-infected individuals, with nearly 2-3 fold greater frequencies of CD4+CD38+ (1.8-fold; p=0.007), CD4+CD38+HLA-DR+ (1.9-fold; p=0.0006), CD8+CD38+ (2.8-fold; p=0.0006), CD8+HLA-DR+ (2-fold; p=0.022) and CD8+CD38+HLA-DR+ (3.6-fold; p<0.0001) cells compared to HIV-uninfected individuals. Overall, this study demonstrates a clear disruption of the pulmonary immune environment during HIV infection, with readily detectable virus and activated T lymphocytes, which may be driven to accumulate by local chemokines.
Keywords: HIV; T cells; activation; cytokines; inflammation; lung.
Copyright © 2021 Bunjun, Soares, Thawer, Müller, Kiravu, Ginbot, Corleis, Murugan, Kwon, von Groote-Bidlingmaier, Riou, Wilkinson, Walzl and Burgers.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- UNAIDS . Fact Sheet HIV Statistics (2020). Available at: https://www.unaids.org/en/resources/fact-sheet.
-
- Meghji J, Miller RF. HIV and the Lung. Med (Baltimore) (2013) 41:435–41. 10.1016/j.mpmed.2013.05.015 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials