

Irreversible Electroporation Treatment With Intraoperative Biliary Stenting for Unresectable Perihilar Cholangiocarcinoma: A Pilot Study
- PMID: 34277454
- PMCID: PMC8278819
- DOI: 10.3389/fonc.2021.710536
Irreversible Electroporation Treatment With Intraoperative Biliary Stenting for Unresectable Perihilar Cholangiocarcinoma: A Pilot Study
Abstract
Background: Treating perihilar cholangiocarcinoma (PHCC) is particularly difficult due to the fact that it is usually in an advanced stage at the time of diagnosis. Irreversible electroporation treatment (IRE) involves the local administration of a high-voltage electric current to target lesions without causing damage to surrounding structures. This study investigated the safety and efficacy of using IRE in conjunction with intraoperative biliary stent placement in cases of unresectable PHCC.
Methods: This study enrolled 17 patients with unresectable Bismuth type III/IV PHCC who underwent IRE in conjunction with intraoperative biliary stent placement (laparotomic) in two medical centers in Asia between June 2015 and July 2018. Analysis focused on the perioperative clinical course, the efficacy of biliary decompression, and outcomes (survival).
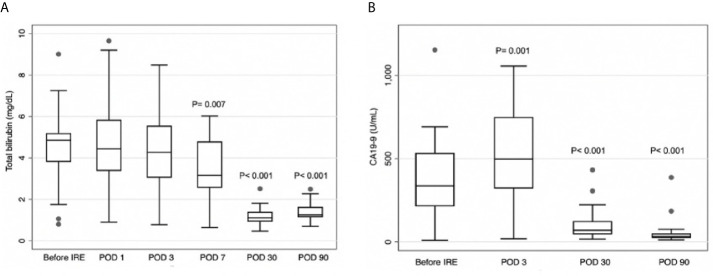
Results: Mean total serum bilirubin levels (mg/dL) on postoperative day (POD) 7, POD30, and POD90 were significantly lower than before IRE (respectively 3.46 vs 4.54, p=0.007; 1.21 vs 4.54, p<0.001; 1.99 vs 4.54, p<0.001). Mean serum carbohydrate antigen 19-9 (CA19-9, U/ml) levels were significantly higher on POD3 than before the operation (518.8 vs 372.4, p=0.001) and significantly lower on POD30 and POD90 (respectively 113.7 vs 372.4, p<0.001; 63.9 vs 372.4, p<0.001). No cases of Clavien-Dindo grade III/IV adverse events or mortality occurred within 90 days post-op. The median progression-free survival was 21.5 months, and the median overall survival was 27.9 months. All individuals who survived for at least one year did so without the need to carry percutaneous biliary drainage (PTBD) tubes.
Conclusions: It appears that IRE treatment in conjunction with intraoperative biliary stent placement is a safe and effective approach to treating unresectable PHCC. The decompression of biliary obstruction without the need for PTBD tubes is also expected to improve the quality of life of patients.
Keywords: Jaundice cholangitis; biliary stent; irreversible electroporation; perihilar cholangiocarcinoma (PHCCA); unresectable abdominal neoplasms.
Copyright © 2021 Yang, Chen, Li, Hsiao, Cheng, Gao, Zhou, Chen, Hu, Zeng and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous