

Use of Almitrine and Inhaled Nitric Oxide in ARDS Due to COVID-19
- PMID: 34277653
- PMCID: PMC8280335
- DOI: 10.3389/fmed.2021.655763
Use of Almitrine and Inhaled Nitric Oxide in ARDS Due to COVID-19
Abstract
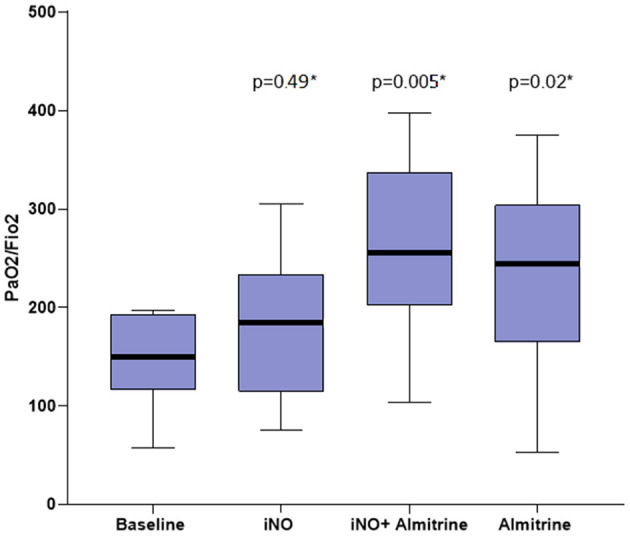
Introduction: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is manifested by an acute respiratory distress syndrome (ARDS) with intense inflammation and endothelial dysfunction leading to particularly severe hypoxemia. We hypothesized that an impaired hypoxic pulmonary vasoconstriction aggravates hypoxemia. The objective of the study was to test the effect of two pulmonary vasoactive drugs on patient oxygenation. Methods: Observational, single-center, open-label study in one intensive care unit (ICU) of the Paris area, realized in April 2020. Eligible patients had coronavirus disease 2019 (COVID-19) and moderate to severe ARDS [arterial partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2) <200 mmHg] despite conventional protective ventilation. Exclusion criteria included pulmonary artery hypertension defined by a pulmonary artery systolic pressure (PAPs) >45 mmHg. The assessment of oxygenation was based on PaO2/FiO2 at (1) baseline, then after (2) 30 min of inhaled nitric oxide (iNO) 10 ppm alone, then (3) 30 min combination of iNO + almitrine infusion 8 μg/kg/min, then (4) 30 min of almitrine infusion alone. Results: Among 20 patients requiring mechanical ventilation during the study period, 12 met the inclusion criteria. Baseline PaO2/FiO2 was 146 ± 48 mmHg. When iNO was combined with almitrine, PaO2/FiO2 rose to 255 ± 90 mmHg (+80 ± 49%, p = 0.005), also after almitrine alone: 238 ± 98 mmHg (+67 ± 75%, p = 0.02), but not after iNO alone: 185 ± 73 mmHg (+30 ± 5%, p = 0.49). No adverse events related to almitrine infusion or iNO was observed. Conclusion: Combining iNO and infused almitrine improved the short-term oxygenation in patients with COVID-19-related ARDS. This combination may be of interest when first-line therapies fail to restore adequate oxygenation. These findings argue for an impaired pulmonary hypoxic vasoconstriction in these patients.
Keywords: COVID-19; acute respiratory distress syndrome; almitrine; mechanical ventilation; nitric oxide.
Copyright © 2021 Laghlam, Rahoual, Malvy, Estagnasié, Brusset and Squara.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Evans PC, Ed Rainger G, Mason JC, Guzik TJ, Osto E, Stamataki Z, et al. . Endothelial dysfunction in COVID-19: a position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc Res. (2020) 116:2177–84. 10.1093/cvr/cvaa230 - DOI - PMC - PubMed
-
- Villar J, Martin-Rodriguez C, Dominguez-Berrot AM, Fernandez L, Ferrando C, Soler JA, et al. . A quantile analysis of plateau and driving pressures: effects on mortality in patients with acute respiratory distress syndrome receiving lung-protective ventilation. Crit Care Med. (2017) 45:843–50. 10.1097/CCM.0000000000002330 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous