

The role of ultrasound in determining the amount of pleural effusion
- PMID: 34277772
- PMCID: PMC8267331
- DOI: 10.21037/atm-21-2214
The role of ultrasound in determining the amount of pleural effusion
Abstract
Background: There is no standardized system to evaluate pleural effusion size on ultrasound (US). We aimed to explore the role of US in determining the amount of pleural effusion, with an attempt to provide evidence for clinical efficacy evaluation and treatment program selection.
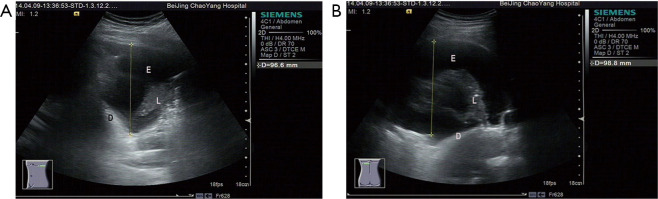
Methods: A total of 98 patients undergoing thoracoscopy at our center were enrolled in this study. The patients take a sitting position, then the maximum depths of the pleural effusion by US at the subscapular line, posterior axillary line, midaxillary line, anterior axillary line, and midclavicular line, as well as the maximum thickness of the pleural effusion at the subscapular line, were measured before pleural effusion drainage. Then, the corresponding values in the lateral position were also measured. The relationships between the actual pleural effusion amounts and the measurements at these lines were analyzed using the multivariate linear regression model (MLRM).
Results: The regression equation of the group with a pleural effusion amount of 500-1,000 mL in the sitting position showed statistical significance (P=0.001). The P values of the maximum depths at the subscapular line (X1) and midclavicular line (X5) and the maximum thickness at the subscapular line (X6) were below 0.05. Thus, a final model was established using X1, X5, and X6 as the independent variables.
Conclusions: The combination of US examination and MLRM enables the quantitative determination of pleural effusion.
Keywords: Pleural effusion; logistic regression; ultrasound (US).
2021 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/atm-21-2214). The authors have no conflicts of interest to declare.
Figures



References
LinkOut - more resources
Full Text Sources