

Pulmonary Sequelae at 4 Months After COVID-19 Infection: A Single-Centre Experience of a COVID Follow-Up Service
- PMID: 34278556
- PMCID: PMC8286847
- DOI: 10.1007/s12325-021-01833-4
Pulmonary Sequelae at 4 Months After COVID-19 Infection: A Single-Centre Experience of a COVID Follow-Up Service
Abstract
Introduction: At the end of the first year of the COVID-19 pandemic, more than 78 million known survivors were recorded. The long-term pulmonary sequelae of COVID-19 remain unknown.
Methods: We performed a retrospective analysis of a post-COVID follow-up service to estimate the burden of persistent pulmonary morbidity in hospitalised COVID survivors.
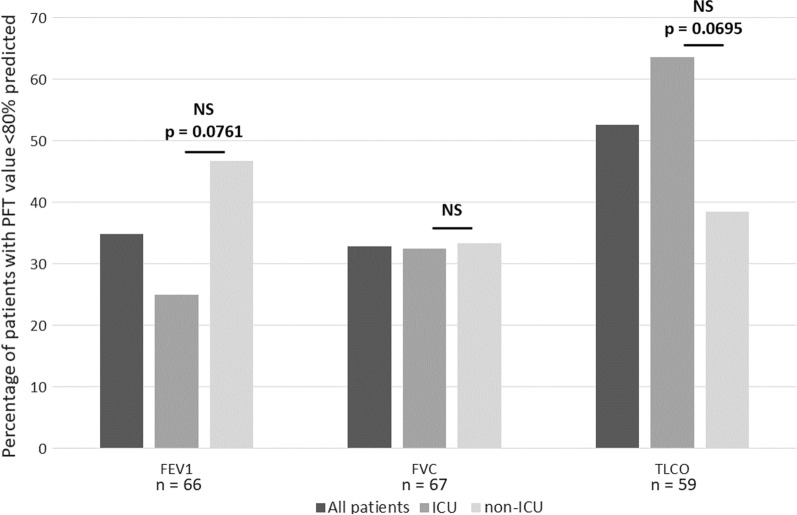
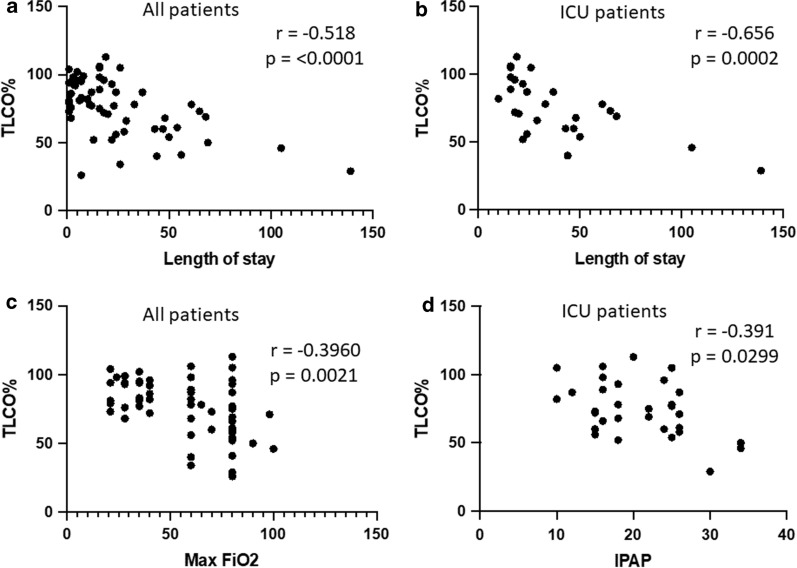
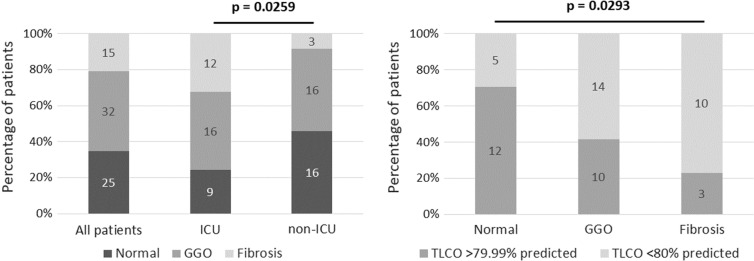
Results: A total of 221 patients were followed-up: 44 intensive care unit (ICU) and 177 ward patients. Further investigations were planned as per British Thoracic Society Guidelines: For all ICU patients (n = 44) and for 38 of 177 (21%) ward-based patients who had persistent symptoms and/or persistent radiographic changes on CXR at their initial 8-week follow-up visit. In the ward-based cohort, statistically significant associations with persistent symptoms were being an ex- or current smoker, having pre-existing diabetes, and having a longer length of stay. In patients requiring further investigations, pulmonary function tests (PFTs; n = 67) at an average of 15 weeks post-discharge showed abnormalities in at least one PFT parameter in 79% (equating to 24% of the entire cohort). The most common abnormality was an abnormal diffusion capacity of carbon monoxide (TLCO), highest in the ICU cohort (64% ICU vs. 38% non-ICU). TLCO correlated negatively with length of stay and with maximum inspired FiO2 in the patient group as a whole. In ICU patients, TLCO correlated negatively with maximum inspired positive airway pressure. Computed tomography scans (n = 72) at an average of 18 weeks post-discharge showed evidence of persistent ground glass opacities in 44% and fibrosis in 21% (equating to 7% of the entire cohort).
Conclusion: Our data add to the growing evidence that there will be pulmonary sequelae in a proportion of COVID survivors, providing some insight into what may become a significant chronic global health problem.
Keywords: COVID-19; Coronavirus; Pulmonary function tests; Pulmonary sequelae; Radiological fibrosis.
© 2021. The Author(s).
Figures
References
-
- https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-ch.... Data extracted 30th December 2020.
-
- https://covid19.who.int. Data extracted 30th December 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
