

International Consensus for the Dosing of Corticosteroids in Childhood-Onset Systemic Lupus Erythematosus With Proliferative Lupus Nephritis
- PMID: 34279063
- PMCID: PMC8766607
- DOI: 10.1002/art.41930
International Consensus for the Dosing of Corticosteroids in Childhood-Onset Systemic Lupus Erythematosus With Proliferative Lupus Nephritis
Abstract
Objective: To develop a standardized steroid dosing regimen (SSR) for physicians treating childhood-onset systemic lupus erythematosus (SLE) complicated by lupus nephritis (LN), using consensus formation methodology.
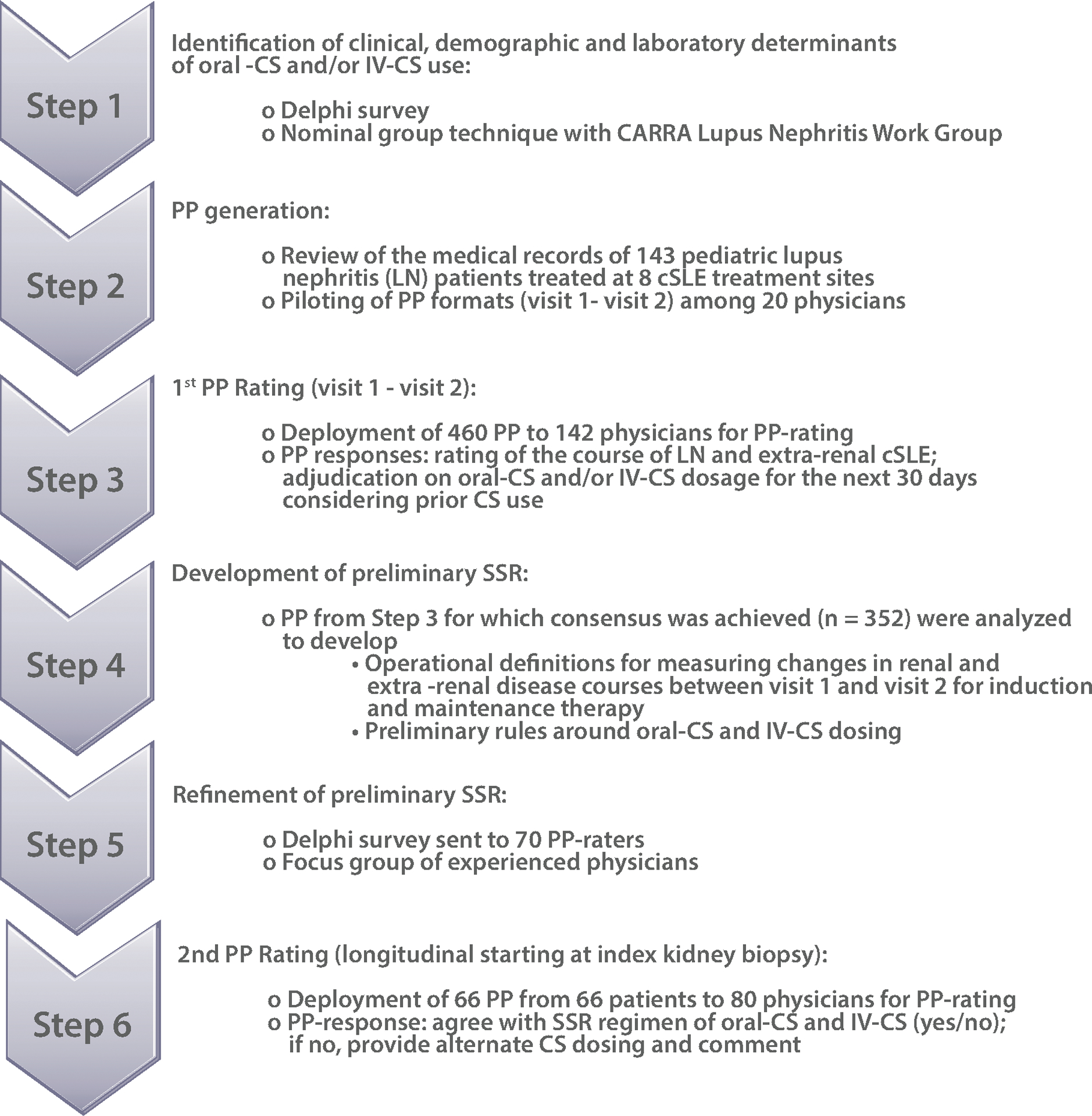
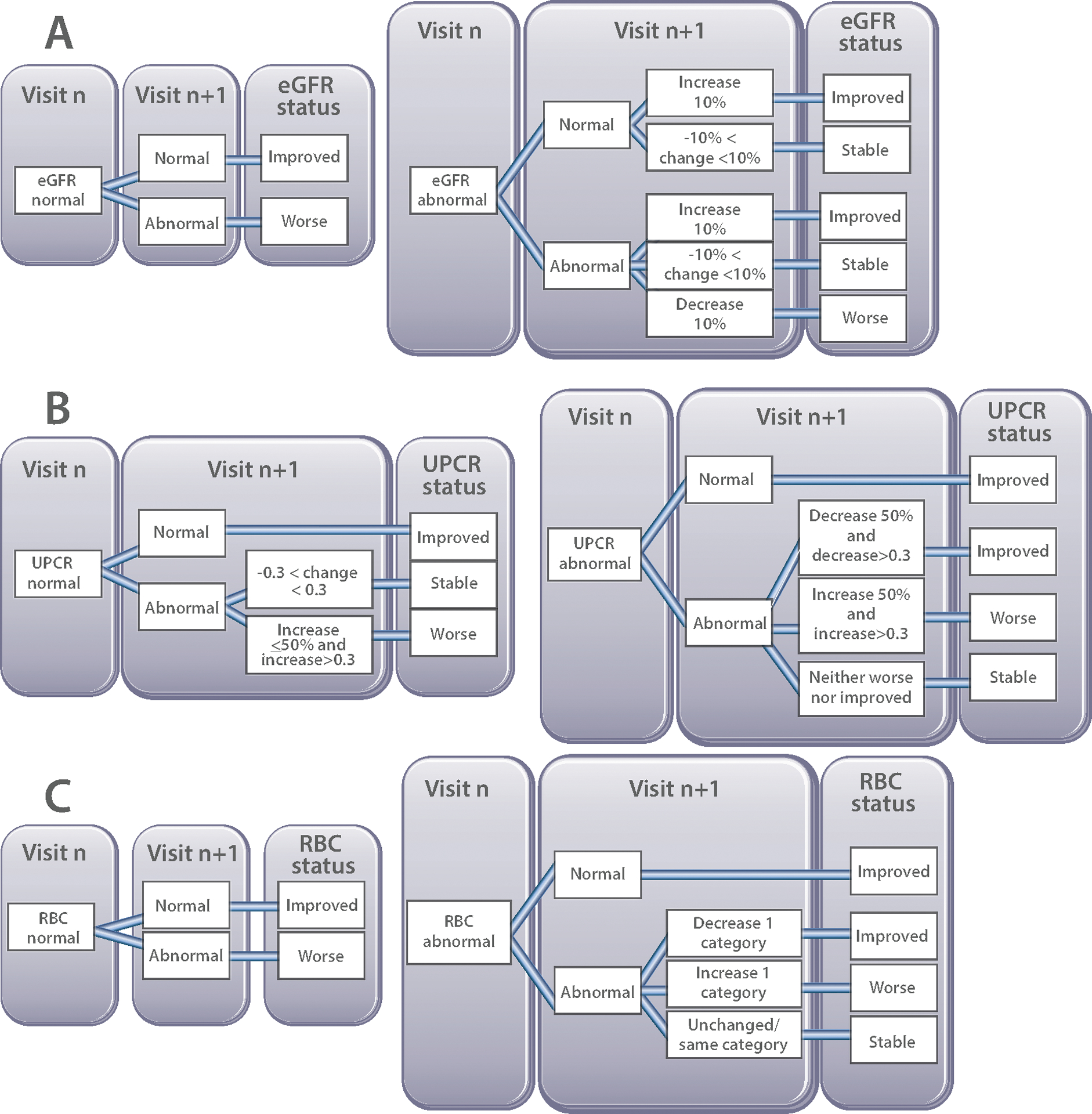
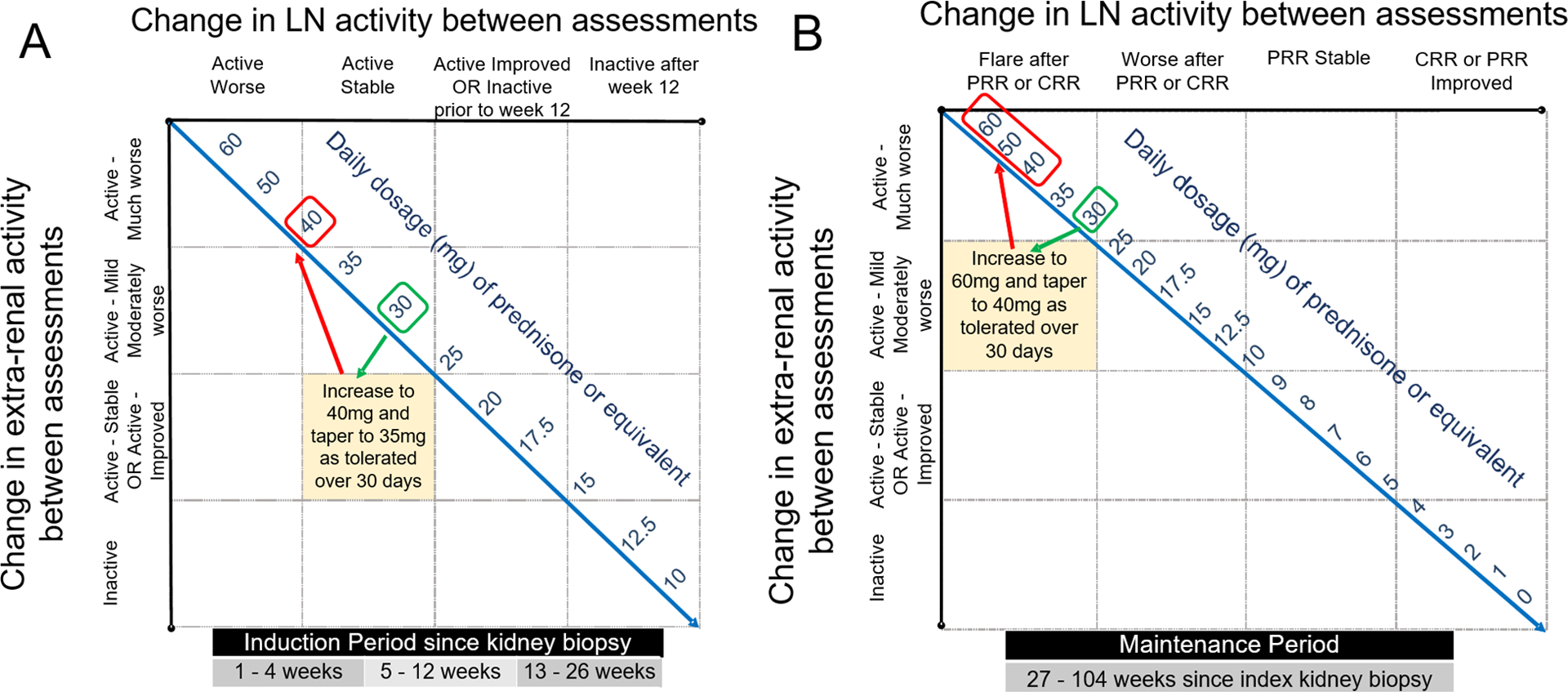
Methods: Parameters influencing corticosteroid (CS) dosing were identified (step 1). Data from children with proliferative LN were used to generate patient profiles (step 2). Physicians rated changes in renal and extrarenal childhood-onset SLE activity between 2 consecutive visits and proposed CS dosing (step 3). The SSR was developed using patient profile ratings (step 4), with refinements achieved in a physician focus group (step 5). A second type of patient profile describing the course of childhood-onset SLE for ≥4 months since kidney biopsy was rated to validate the SSR-recommended oral and intravenous (IV) CS dosages (step 6). Patient profile adjudication was based on majority ratings for both renal and extrarenal disease courses, and consensus level was set at 80%.
Results: Degree of proteinuria, estimated glomerular filtration rate, changes in renal and extrarenal disease activity, and time since kidney biopsy influenced CS dosing (steps 1 and 2). Considering these parameters in 5,056 patient profile ratings from 103 raters, and renal and extrarenal course definitions, CS dosing rules of the SSR were developed (steps 3-5). Validation of the SSR for up to 6 months post-kidney biopsy was achieved with 1,838 patient profile ratings from 60 raters who achieved consensus for oral and IV CS dosage in accordance with the SSR (step 6).
Conclusion: The SSR represents an international consensus on CS dosing for use in patients with childhood-onset SLE and proliferative LN. The SSR is anticipated to be used for clinical care and to standardize CS dosage during clinical trials.
© 2021, American College of Rheumatology.
Figures
References
-
- Brunner HI, Klein-Gitelman MS, Ying J, Tucker LB, Silverman ED. Corticosteroid use in childhood-onset systemic lupus erythematosus-practice patterns at four pediatric rheumatology centers. Clin Exp Rheumatol. 2009;27(1):155–62. - PubMed
-
- Criteria for steroid-sparing ability of interventions in systemic lupus erythematosus: report of a consensus meeting. Arthritis and rheumatism. 2004;50(11):3427–31. - PubMed
-
- Cooper JC, Rouster-Stevens K, Wright TB, Hsu JJ, Klein-Gitelman MS, Ardoin SP, et al. Pilot study comparing the childhood arthritis and rheumatology research alliance consensus treatment plans for induction therapy of juvenile proliferative lupus nephritis. Pediatr Rheumatol Online J. 2018;16(1):65. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000445/TR/NCATS NIH HHS/United States
- BRC 525 III/CC/NIHR University College London Hospitals Biomedical Research Centre
- Beijing Municipal Bureau of Foreign Affairs Training
- T32-AR-050958/National Center for Advancing Translational Sciences, NIH
- P50-DK-096418/DK/NIDDK NIH HHS/United States
- Pediatric Musculoskeletal & Rheumatology Innovation Core center (PORTICO)
- 303422/2015-7/Conselho Nacional de Desenvolvimento Científico e Tecnológico
- UL1 TR000077/TR/NCATS NIH HHS/United States
- Núcleo de Apoio à Pesquisa "Saúde da Criança e do Adolescente" da USP
- R34-AR-071651/National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS]
- FAPESP 2015/03756-4/Fundação de Amparo à Pesquisa do Estado de São Paulo
- P30 AR076316/AR/NIAMS NIH HHS/United States
- P30-AR-076316/National Institute of Arthritis and Musculoskeletal and Skin Diseases [NIAMS]
- R34 AR071651/AR/NIAMS NIH HHS/United States
- P50 DK096418/DK/NIDDK NIH HHS/United States
- T32 AR050958/AR/NIAMS NIH HHS/United States
- 21593/Centre for Adolescent Rheumatology Versus Arthritis
- Arthritis Foundation
- UL1 TR001425/TR/NCATS NIH HHS/United States
- Institutional Clinical and Translational Science
- P50-DK-096418/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
