

Association of Adverse Events With Antibiotic Treatment for Urinary Tract Infection
- PMID: 34279560
- PMCID: PMC9049277
- DOI: 10.1093/cid/ciab637
Association of Adverse Events With Antibiotic Treatment for Urinary Tract Infection
Abstract
Background: Little is known about the relative harms of different antibiotic regimens prescribed to treat uncomplicated urinary tract infection (UTI). We sought to compare the risk of adverse events associated with commonly used oral antibiotic regimens for the outpatient treatment of uncomplicated UTI.
Methods: Using data from the IBM® MarketScan® Commercial Database, we identified 1 169 033 otherwise healthy, nonpregnant women aged 18-44 years with uncomplicated UTI who initiated an oral antibiotic with activity against common uropathogens from 1 July 2006 to 30 September 2015. We used propensity score-weighted Kaplan-Meier methods and Cox proportional hazards regression models to estimate the association between antibiotic agent and adverse events.
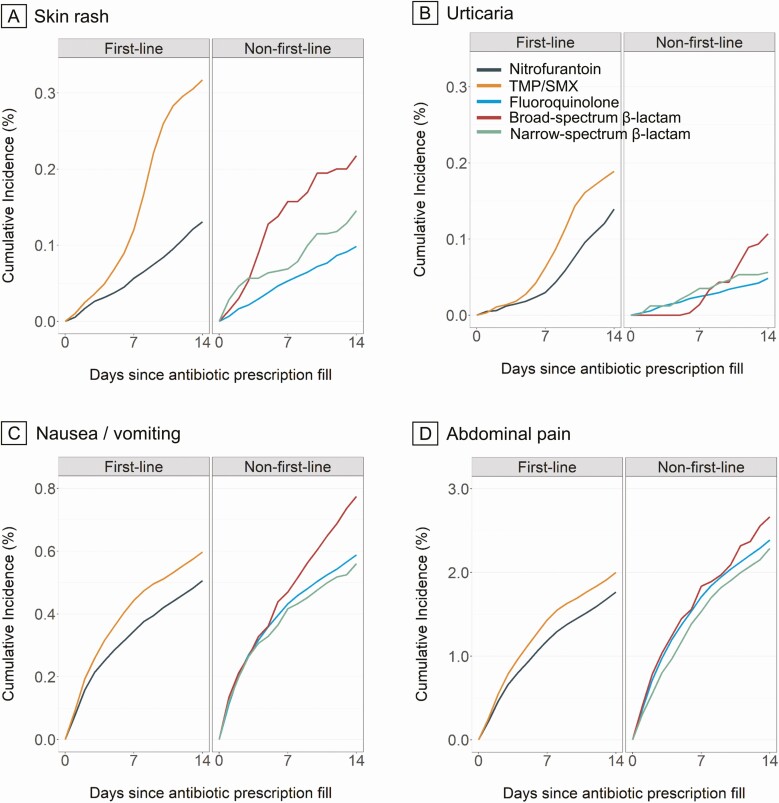
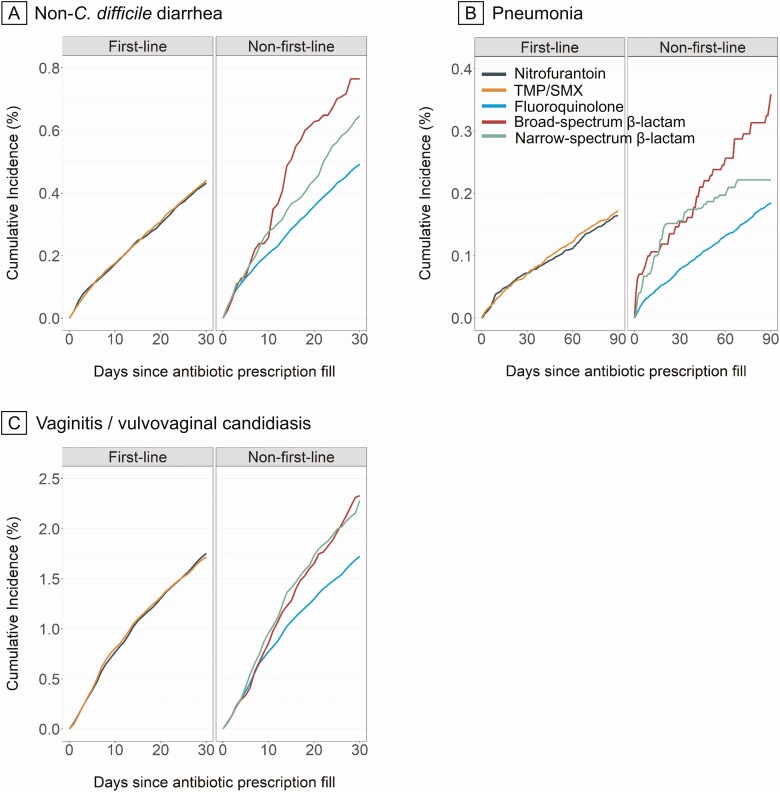
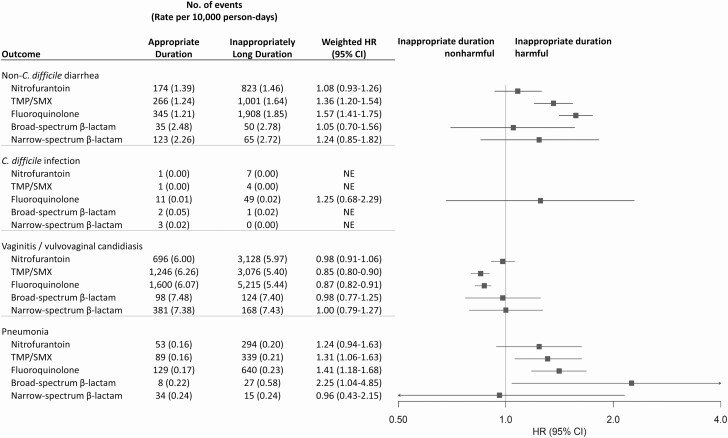
Results: Of 2 first-line agents, trimethoprim-sulfamethoxazole (vs nitrofurantoin) was associated with higher risk of several adverse drug events including hypersensitivity reaction (hazard ratio, 2.62; 95% confidence interval, 2.30-2.98), acute renal failure (2.56; 1.55-4.25), skin rash (2.42; 2.13-2.75), urticaria (1.37; 1.19-1.57), abdominal pain (1.14; 1.09-1.19), and nausea/vomiting (1.18; 1.10-1.28), but a similar risk of potential microbiome-related adverse events. Compared with nitrofurantoin, non-first-line agents were associated with higher risk of several adverse drug events and potential microbiome-related adverse events including non-Clostridium difficile diarrhea, C. difficile infection, vaginitis/vulvovaginal candidiasis, and pneumonia. Treatment duration modified the risk of potential microbiome-related adverse events.
Conclusions: The risks of adverse drug events and potential microbiome-related events differ widely by antibiotic agent and duration. These findings underscore the utility of using real-world data to fill evidentiary gaps related to antibiotic safety.
Keywords: administrative data; adverse events; antibiotics; comparative safety; urinary tract infection.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Hicks LA, Bartoces MG, Roberts RM, et al. . US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis 2015; 60:1308–16. - PubMed
-
- Gupta K, Hooton TM, Naber KG, et al. . International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011; 52:e103–20. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. . Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016; 315:1864–73. - PubMed
-
- Grigoryan L, Trautner BW, Gupta K. Diagnosis and management of urinary tract infections in the outpatient setting: a review. JAMA 2014; 312: 1677–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
