

Do psychiatric diseases follow annual cyclic seasonality?
- PMID: 34280189
- PMCID: PMC8345894
- DOI: 10.1371/journal.pbio.3001347
Do psychiatric diseases follow annual cyclic seasonality?
Abstract
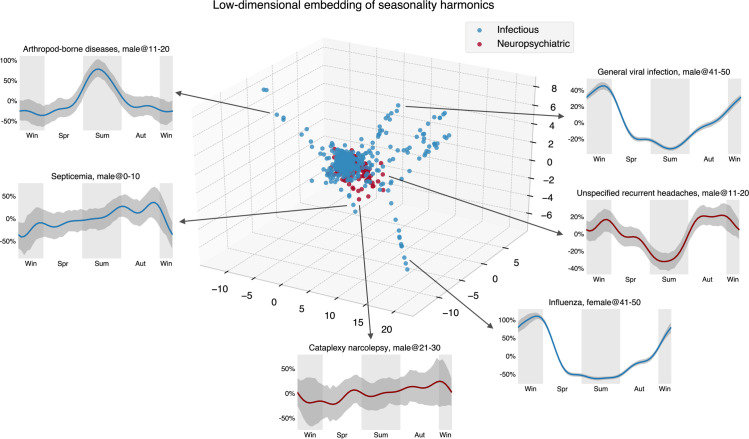
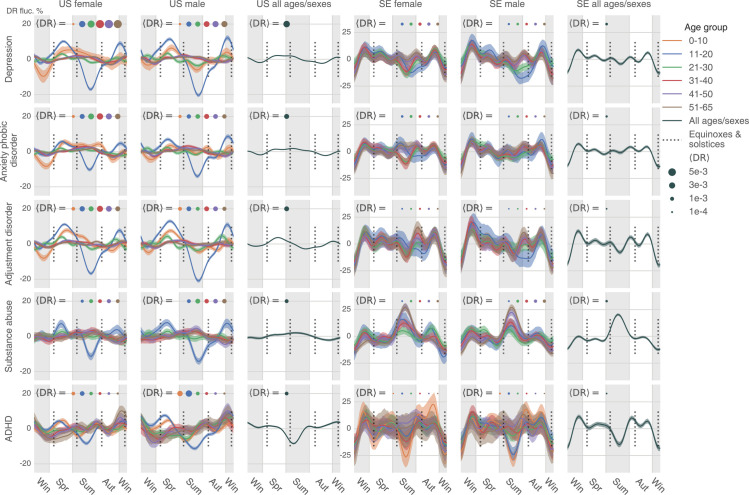
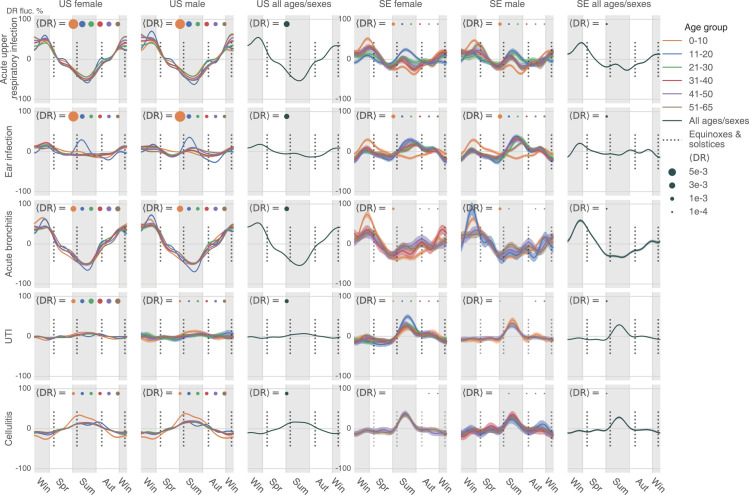
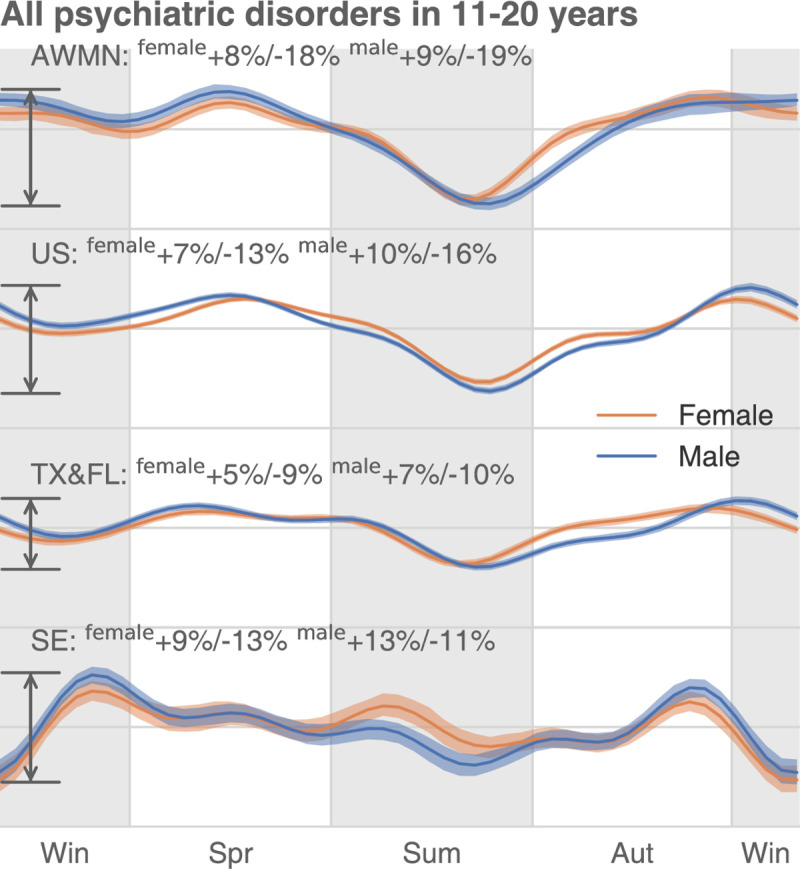
Seasonal affective disorder (SAD) famously follows annual cycles, with incidence elevation in the fall and spring. Should some version of cyclic annual pattern be expected from other psychiatric disorders? Would annual cycles be similar for distinct psychiatric conditions? This study probes these questions using 2 very large datasets describing the health histories of 150 million unique U.S. citizens and the entire Swedish population. We performed 2 types of analysis, using "uncorrected" and "corrected" observations. The former analysis focused on counts of daily patient visits associated with each disease. The latter analysis instead looked at the proportion of disease-specific visits within the total volume of visits for a time interval. In the uncorrected analysis, we found that psychiatric disorders' annual patterns were remarkably similar across the studied diseases in both countries, with the magnitude of annual variation significantly higher in Sweden than in the United States for psychiatric, but not infectious diseases. In the corrected analysis, only 1 group of patients-11 to 20 years old-reproduced all regularities we observed for psychiatric disorders in the uncorrected analysis; the annual healthcare-seeking visit patterns associated with other age-groups changed drastically. Analogous analyses over infectious diseases were less divergent over these 2 types of computation. Comparing these 2 sets of results in the context of published psychiatric disorder seasonality studies, we tend to believe that our uncorrected results are more likely to capture the real trends, while the corrected results perhaps reflect mostly artifacts determined by dominantly fluctuating, health-seeking visits across a given year. However, the divergent results are ultimately inconclusive; thus, we present both sets of results unredacted, and, in the spirit of full disclosure, leave the verdict to the reader.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Solberg BS, Zayats T, Posserud MB, Halmoy A, Engeland A, Haavik J, et al. Patterns of Psychiatric Comorbidity and Genetic Correlations Provide New Insights Into Differences Between Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder. Biol Psychiatry. 2019;86(8):587–98. Epub 2019/06/12. doi: 10.1016/j.biopsych.2019.04.021 ; PubMed Central PMCID: PMC6764861. - DOI - PMC - PubMed
-
- Tylee DS, Sun J, Hess JL, Tahir MA, Sharma E, Malik R, et al. Genetic correlations among psychiatric and immune-related phenotypes based on genome-wide association data. Am J Med Genet B Neuropsychiatr Genet. 2018;177(7):641–57. Epub 2018/10/17. doi: 10.1002/ajmg.b.32652 ; PubMed Central PMCID: PMC6230304. - DOI - PMC - PubMed
-
- Wen Y, Zhang F, Ma X, Fan Q, Wang W, Xu J, et al. eQTLs Weighted Genetic Correlation Analysis Detected Brain Region Differences in Genetic Correlations for Complex Psychiatric Disorders. Schizophr Bull. 2019;45(3):709–15. Epub 2018/06/19. doi: 10.1093/schbul/sby080 ; PubMed Central PMCID: PMC6483588. - DOI - PMC - PubMed
-
- Jia G, Li Y, Zhang H, Chattopadhyay I, Boeck Jensen A, Blair DR, et al. Estimating heritability and genetic correlations from large health datasets in the absence of genetic data. Nat Commun. 2019;10(1):5508. Epub 2019/12/05. doi: 10.1038/s41467-019-13455-0 ; PubMed Central PMCID: PMC6890770. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
