

Evolution of practice patterns in the management of acute respiratory distress syndrome: A secondary analysis of two successive randomized controlled trials
- PMID: 34280657
- PMCID: PMC8255112
- DOI: 10.1016/j.jcrc.2021.06.017
Evolution of practice patterns in the management of acute respiratory distress syndrome: A secondary analysis of two successive randomized controlled trials
Abstract
Purpose: We sought to examine changes in acute respiratory distress syndrome (ARDS) management over a 12-year period of two successive randomized trials.
Methods: Analyses included baseline data, from eligible patients, prior to influence of trial protocols, and daily study data, from randomized patients, of variables not determined by trial protocols. Mixed linear regressions examined changes in practice year-on-year.
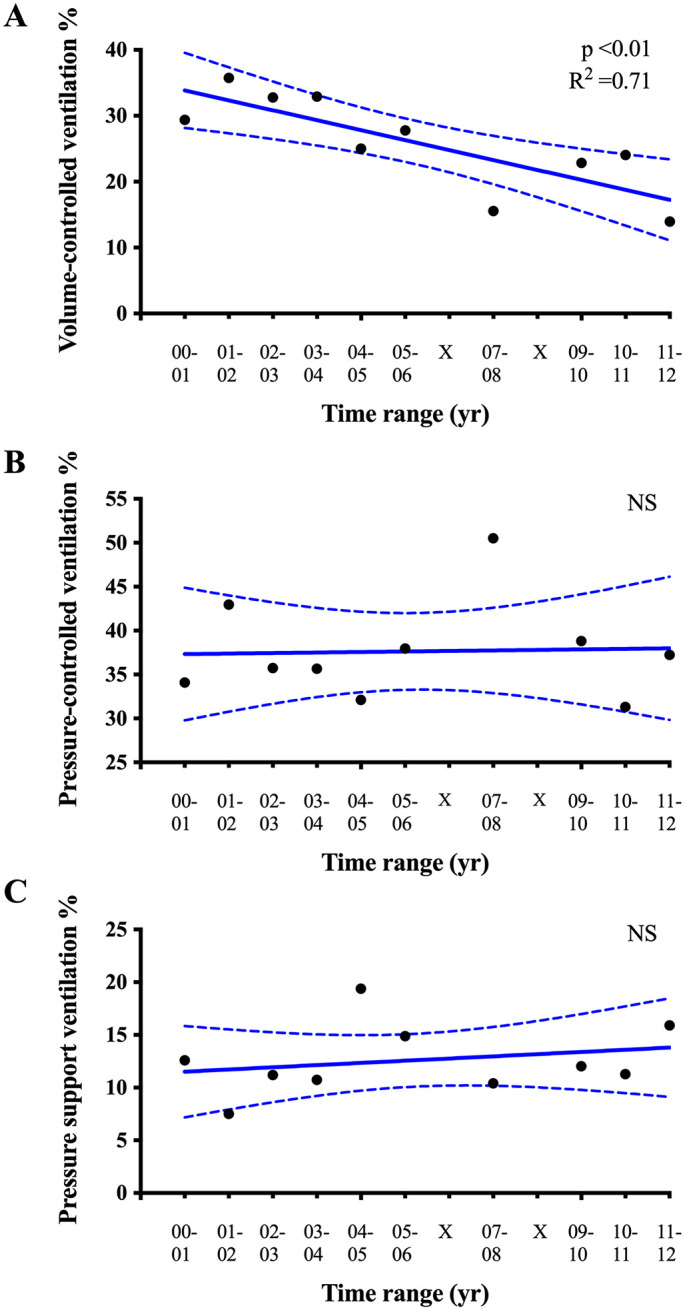
Results: A total of 2376 patients met the inclusion criteria. Over the 12-year period, baseline tidal volume index decreased (9.0 to 7.0 ml/kg, p < 0.001), plateau pressures decreased (30.8 to 29.0 cmH2O, p < 0.05), and baseline positive end-expiratory pressures increased (10.8 to 13.2 cmH2O, p < 0.001). Volume-controlled ventilation declined from 29.4 to 14.0% (p < 0.01). Use of corticosteroids increased (baseline: 7.7 to 30.3%; on study: 32.6 to 61.2%; both p < 0.001), as did neuromuscular blockade (baseline: 12.3 to 24.5%; on study: 55.5 to 70.0%; both p < 0.01). Inhaled nitric oxide use increased (24.9 to 65.8%, p < 0.05). We observed no significant change in prone positioning (16.2 to 18.9%, p = 0.70).
Conclusions: Clear trends were apparent in tidal volume, airway pressures, ventilator modes, adjuncts and rescue therapies. With the exception of prone positioning, and outside the context of rescue therapy, these trends appear consistent with the evolving literature on ARDS management.
Keywords: ARDS; Corticosteroid; High frequency oscillatory ventilation; Inhaled nitric oxide; Mechanical ventilation; Neuromuscular blockade; PEEP; Plateau pressure; Tidal volume; Volume-controlled ventilation.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest All the other authors declare no conflicts of interest.
Figures



References
-
- Network Acute Respiratory Distress Syndrome, Brower R.G., Matthay M.A., Morris A., Schoenfeld D., Thompson B.T., et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
-
- Serpa Neto A., Cardoso S.O., Manetta J.A., Pereira V.G., Esposito D.C., Pasqualucci Mde O., et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;308(16):1651–1659. doi: 10.1001/jama.2012.13730. - DOI - PubMed
-
- Goligher E.C., Kavanagh B.P., Rubenfeld G.D., Adhikari N.K., Pinto R., Fan E., et al. Oxygenation response to positive end-expiratory pressure predicts mortality in acute respiratory distress syndrome. A secondary analysis of the LOVS and ExPress trials. Am J Respir Crit Care Med. 2014;190(1):70–76. doi: 10.1164/rccm.201404-0688OC. - DOI - PubMed
-
- Briel M., Meade M., Mercat A., Brower R.G., Talmor D., Walter S.D., et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010;303(9):865–873. doi: 10.1001/jama.2010.218. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
