

Coronavirus disease 2019 vaccine mimics lymph node metastases in patients undergoing skin cancer follow-up: A monocentre study
- PMID: 34280870
- PMCID: PMC8233908
- DOI: 10.1016/j.ejca.2021.06.023
Coronavirus disease 2019 vaccine mimics lymph node metastases in patients undergoing skin cancer follow-up: A monocentre study
Abstract
Introduction: The coronavirus disease 2019 (COVID-19) pandemic has changed the lives of people around the world. Fortunately, sufficient vaccines are now available. Local reactions with ipsilateral lymphadenopathy are among the most common side effects. We investigated the impact of lymphadenopathy after COVID-19 vaccination on the value of ultrasound in tumour patients.
Patients and methods: Patients with melanoma or Merkel cell carcinoma were included who underwent lymph node excision and received COVID-19 vaccination within 6 weeks before surgery. The consistency of the preoperative ultrasound findings with the histopathologic findings was investigated.
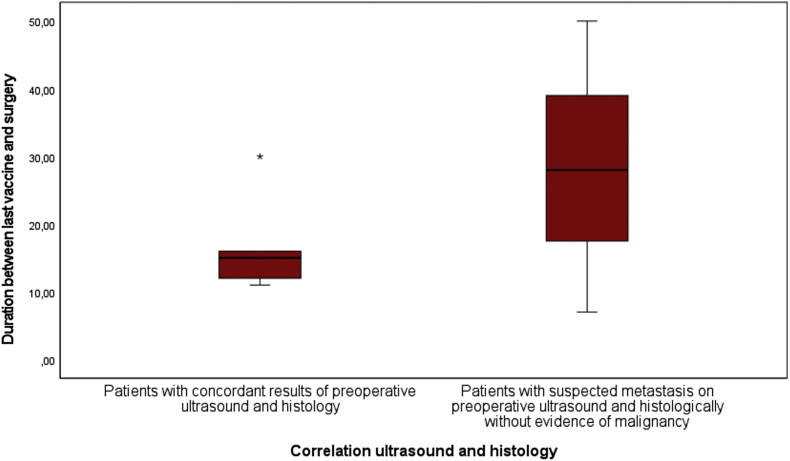
Results: Eight patients were included (two Merkel cell carcinoma and six melanoma patients) who underwent lymph node excision between 16th April 2021 and 19th May 2021 and had previously received COVID-19 vaccination. In three of the eight patients (one Merkel cell carcinoma and two melanoma patients), lymph node metastases were erroneously diagnosed preoperatively during tumour follow-up with physical examination, ultrasound, and or fluorodeoxyglucose (FDG)-positron emission tomography (PET)/computed tomography (CT). In these three patients, the suspected lymph node metastases were located in the left axilla after COVID-19 vaccination in the left upper arm, which resulted in selective lymph node removal in two patients and complete lymphadenectomy in one patient.
Conclusion: COVID-19 vaccine-associated lymphadenopathy is expected to be observed much more frequently in the near future because of increasing vaccination rates. This cause of lymphadenopathy, which may in ultrasound as well as in FDG PET/CT resemble lymph node metastases, must be considered, especially in oncologic patients undergoing tumour follow-up. In addition, COVID-19 vaccination should be given as far away as possible from an underlying primary on the contralateral side to avoid oncologic misdiagnosis followed by malpractice.
Keywords: COVID-19 vaccine; Lymphadenopathy; Melanoma; Merkel cell carcinoma; Ultrasound.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement J.M.P. served as consultant and/or has received honoraria from Bristol-Myers Squibb and Novartis and has received travel support from Bristol-Myers Squibb, Novartis, and Therakos. J.K. reported grants and or personal fees from Novartis, LaVision Bio Tec, and SastoMed. A.R. reported grants from Novartis, Bristol Myers Squibb, and ADTEC; personal fees from Merck Sharp & Dohme; and nonfinancial support from Amgen, Roche, Merck Sharp & Dohme, Novartis, Bristol Myers Squibb, and Teva. D.S. received grants and other support from Bristol-Myers Squibb, personal fees from Bristol-Myers Squibb during the conduct of the study; personal fees from Amgen; personal fees from Boehringer Ingelheim; personal fees from InFlarX; personal fees and other support from Roche; grants, personal fees, and other support from Novartis; personal fees from Incyte; personal fees and other support from Regeneron; personal fees from 4SC; personal fees from Sanofi; personal fees from NeraCare; personal fees from Pierre-Fabre; personal fees and other support from Merck-EMD; personal fees from Pfizer; personal fees and other support from Philogen; personal fees from Array; and personal fees and other support from MSD Sharp & Dohme, outside the submitted work. H.R. is on the advisory board of Bristol-Myers Squibb, received honoraria from Roche and Bristol-Myers Squibb, received travel support from Philips, Roche, and Bristol-Myers Squibb, received grants from Bristol-Myers Squibb, and holds shares of Bayer. I.S. and E.H. declared that they have no conflicts of interest with respect to the authorship or the publication of this article.
Figures

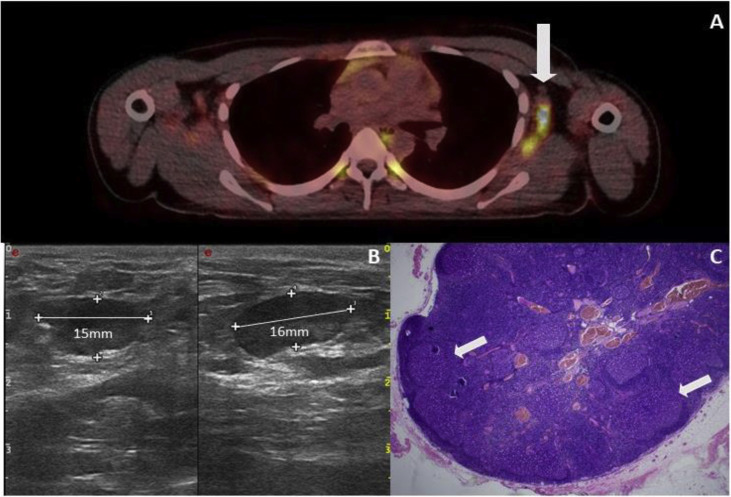
 ). (B) Lymph node ultrasound shows pronounced enlargement with a clear decrease in echogenicity. (C) Histological picture of the lymph node showing follicular hyperplasia (). Metastases from the melanoma cannot be seen (HE).
). (B) Lymph node ultrasound shows pronounced enlargement with a clear decrease in echogenicity. (C) Histological picture of the lymph node showing follicular hyperplasia (). Metastases from the melanoma cannot be seen (HE).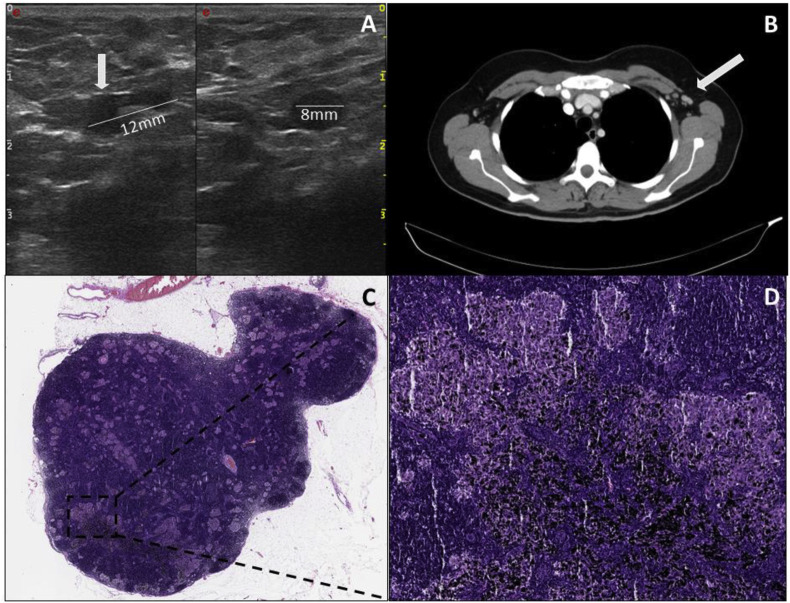 ). (C) Histopathologic image of the lymph node. (D)The sarcoidosis-like granulomas/lesions are visible in addition to distinct pigmentary deposits associated with the patient's underlying tattooing.
). (C) Histopathologic image of the lymph node. (D)The sarcoidosis-like granulomas/lesions are visible in addition to distinct pigmentary deposits associated with the patient's underlying tattooing.References
-
- Larkin J., et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535–1546. - PubMed
-
- Migden M.R., et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379(4):341–351. - PubMed
-
- Hausmann D., et al. Comparison of the diagnostic accuracy of whole-body MRI and whole-body CT in stage III/IV malignant melanoma. J Dtsch Dermatol Ges. 2011;9(3):212–222. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
