

A case report of gallbladder cancer and pancreas cystic neoplasm associated with pancreaticobiliary maljunction
- PMID: 34280877
- PMCID: PMC8319447
- DOI: 10.1016/j.ijscr.2021.106170
A case report of gallbladder cancer and pancreas cystic neoplasm associated with pancreaticobiliary maljunction
Abstract
Introduction and importance: Pancreaticobiliary maljunction (PBM) is a rare congenital anomaly that is frequently associated with carcinoma of the biliary tract. However, there is still no clear evidence that PBM is associated with pancreatic tumors. Here we describe a case of gallbladder cancer and intraductal papillary mucinous neoplasm (IPMN) that is associated with PBM.
Case presentation: A 72-year-old man underwent a cholecystectomy with hepatectomy (S4a + S5) and regional lymph node dissection for gallbladder adenocarcinoma invading the front lobe branch of the hepatic artery. A pylorus-preserving pancreaticodudenectomy was also performed for pancreatic IPMN.
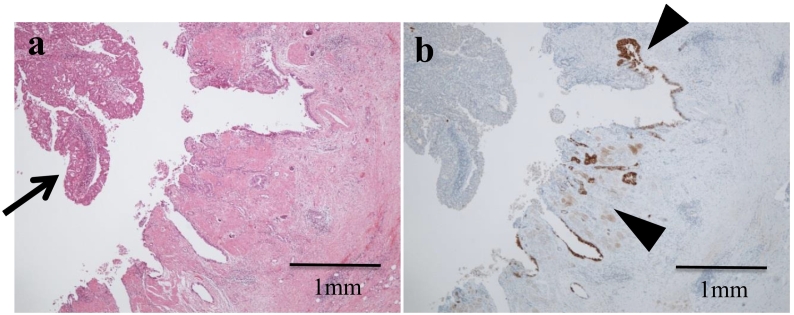
Clinical discussion: Presence of mucin type 6 (MUC6) -positive pyloric gland metaplasia in both the dilated pancreatic duct and the gallbladder background mucosa suggests that pancreatic IPMN and gallbladder cancer may have a common phenotypic origin. Additionally, analysis of 41 reported cases of pancreatic cancer associated with PBM revealed that in all metachronous multiple cancer cases, biliary tract cancer preceded the pancreatic cancer with congenital biliary dilatation accompanied by PBM. The analysis also revealed an increased proportion of pancreatic cancer cases with PBM in patients who had not undergone a flow diversion procedure located in pancreatic head.
Conclusion: We show an interesting relationship between pancreatic/gallbladder cancer and PBM. More comprehensive evaluations of the whole pancreaticobiliary system in follow-up of patients with PBM is required to understand the full extent of this relationship.
Keywords: Case report; Gallbladder cancer; Intraductal papillary mucinous neoplasm; Pancreaticobiliary maljunction.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Yamao K., Mizutani S., Nakazawa S., Inui K., Kanemaki N., Miyoshi H., Segawa K., Zenda H., Kato T. Prospective study of the detection of anomalous connection of pancreatobiliary ducts during routine medical examinations. Hepato-Gastroenterology. 1996;43:1238–1245. - PubMed
-
- Hasumi A., Matsui H., Sugioka A., Uyama I., Komori Y., Fujita J., Aoki H. Precancerous conditions of biliary tract cancer in patients with pancreaticobiliary maljunction: reappraisal of nationwide survey in Japan. J. Hepato-Biliary-Pancreat. Surg. 2000;7:551–555. - PubMed
-
- Kamisawa T., Ando H., Hamada Y., Fujii H., Koshinaga T., Urushihara N., Itoi T. Diagnostic criteria for pancreaticobiliary maljunction. Tando. 2013;27(5):785–787. (in Japanese with English abstract) - PubMed
-
- Funabiki T., Sugiue K., Matsubara T., Amano H., Ochiai M. Bile acids and biliary carcinoma in pancreaticobiliary maljunction. Keio J. Med. 1991;40(3):118–122. - PubMed
LinkOut - more resources
Full Text Sources
